Art of Medicine
Jun 2020

This article reflects on one health care professional’s experience of sitting for Mark Gilbert’s arts-based Patient and Caregiver Portraiture study. The author, a clinical social worker, discusses the roles of ageism, invisibility, and stigma in the lives of people with dementia. This article also explores the similarity between the process of an artist seeing the entirety of a scene and the process of a clinician assessing a patient; both artist and clinician are powerfully influential in their capacity to represent the personhood of a subject or patient.
When artist Mark Gilbert asked that I, a health care professional, reserve an hour in my workday to sit for a life-sized portrait as part of his art-based study on dementia and caregiving, it was not as unusual an “ask” as one might think. For the Geriatric Ambulatory Care/Memory Disability Clinic, part of the Nova Scotia Health Authority (formerly Capital Health), with which I am affiliated, is like a small gallery of local artists’ large oil paintings and sculptures on themes of memory and dementia. This is the result of an artist-in-residence (AIR) program,1 a scholarship program in which artists help assess patients’ memory with families and clinicians and create works that represent what they saw, heard, and felt during that encounter.
The AIR program was inspired by a somber oil painting, Ghost, by Jennifer Hiscox, whose father had early onset dementia. This painting hangs outside my office door and is visited and discussed regularly by people passing by. Ghost is based on a photograph of Hiscox as a young girl; she is in a wading pool and a father figure is scratched out. The photo, taken prior to her father’s diagnosis, shows him looking at Jennifer “like fathers should look at daughters.” Hiscox, feeling not quite able to capture this moment, obscured his image to represent her father as a ghost.2
In what follows, I consider the roles of invisibility, ageism, and stigma in the lives of people with dementia and explore similarities between the process of an artist seeing the entirety of a scene and the process of a clinician assessing a patient.
I am fortunate to spend time outside of work with a social circle of filmmakers, writers, and musicians who identify as working artists. We have a complementary connection. An introvert by nature, I am relieved to sit back and take in all their fascinating discussions in the comfort of knowing that I will not be expected to start a conversation.
I recall one dinner party that changed everything. We were engaging in a typical roundtable discussion about inspiration, process, and grant deadlines, when one of the guests asked about my day. Being more listener than speaker and shy about interjecting myself into their conversation, I quietly offered that I made a home visit with a physician colleague to a retired man who was bedbound and experiencing the end stages of Lewy body dementia. While the physician examined him, I spoke with the patient’s adult son about his conflicting feelings of grief and mixed relief at his father’s imminent death. The disease had so altered his father’s personality that he had not been recognizable for years.
The table fell silent for an uncomfortably long time until someone stated, “We make art about what you do!” Since that time, I have become more aware of “the art” in everyday interactions in my social work practice and have embraced how crucial creativity is when working in the area of memory and dementia care. Mark Gilbert’s Patient and Caregiver Portraiture study has contributed to this awareness.
For more than 20 years, Gilbert has been using portraiture to investigate ideas about care and caregiving. According to Aita et al: “Portraits are introspective in nature implying the ‘interior’ of subject’s experiences.”3 Caregiver portraits in particular reveal the caregiver’s “commitment to care.” More generally, the portraits of patients and caregivers reveal “the centrality of the idea of mortality, the presence of hope despite adversity.”3 Gilbert’s project in the memory clinic is to use life-size pastel portraits of people living with dementia to better understand what they—and those who care for them—are going through.
Being the subject of a portrait was originally unsettling for me and made me feel vulnerable. It is uncommon to be looked at for long periods of time while remaining still. Yet Serbian performance artist Marina Abramović did just that, at a 2010 Museum of Modern Art performance, The Artist Is Present, which was in a sense a social experiment.
Seated silently at a wooden table across from an empty chair, she waited as people took turns sitting in the chair and locking eyes with her. Over the course of nearly three months, for eight hours a day, she met the gaze of 1,000 strangers, many of whom were moved to tears.4
Being seen can create a 2-way empathy connection. As Fogh writes, “being seen feels like unconditional acceptance and belonging,” which “is ultimately exactly what most of us crave.”5
Artists are thought to see the world differently than others because they can train their eye to focus on the details of the entire scene to reveal the person or object.
Unfortunately, Western society’s focus on youth means that older adults are underrepresented in mainstream media.6 When they are portrayed, it is most often negatively, as a generic stereotype or as a comic side gag.7 Older women, in particular, report being unseen and undervalued in society.8 It is so much the case that the “invisible woman” can be anyone, even the famous.9
It wasn’t until I entered the field of geriatrics that I became aware of the societal effects of ageism and was forced to confront ageist attitudes of my own. Even the social work curriculum, which emphasizes social justice for prejudice and discrimination on the basis of race and sex, barely addresses ageism and its potentially drastic effects on older people.10 A Canadian study found that ageism is the most tolerated form of social prejudice—more so than racism and sexism.11 It noted that many well-intentioned people deprive older adults of the independence and choice that are crucial for aging well. In another Canadian study, the author of the present paper and colleagues found that staff members’ low level of risk tolerance towards older adults resulted in older adults not returning home from the hospital as they wished but instead being funneled into nursing homes for their own safety.12
People with dementia must cope in addition with a negative label or social stigma associated with a dementia diagnosis. The general public and many health care professionals have little knowledge of dementia prevention and treatment until a family member develops its signs and symptoms.13,14,15 It is not widely understood that memory loss and other cognitive impairments become defining of a person when they interfere with a person’s ability to function in everyday activities. In the memory clinic where I work, when a patient or family member first receives a diagnosis of dementia, it is common to notice fear and grief as the person’s mind immediately jumps to the end stage of the disease. Many question the ability of persons diagnosed with dementia to care for themselves, make their own decisions, and lead a meaningful life. They are not people living with dementia but demented—labeled by the disease and possibly seen as incompetent, incapable, and a nonperson.
The invisibility of the aged and people with dementia is the backdrop for Gilbert’s Patient and Caregiver Portraiture study. Gilbert’s portable art studio is old school—replete with canvas, easel, and pastels. The warmth of his Scottish burr conveys intimacy and encourages an unburdening of secrets. This artist is very much present, and his subjects feel that he captures their essence while creating their physical likeness.
It was not until my second portrait sitting that I considered the vulnerable position Mark was in, as I watched him in his intimate moment of creating. I immediately asked if I could capture this moment with my cell phone camera and created a photo I call “Me, Looking at You, Looking at Me.” I was pleased when Gilbert said that no one had taken his photo before.
Figure. Kathryn, by Mark Gilbert, 2019
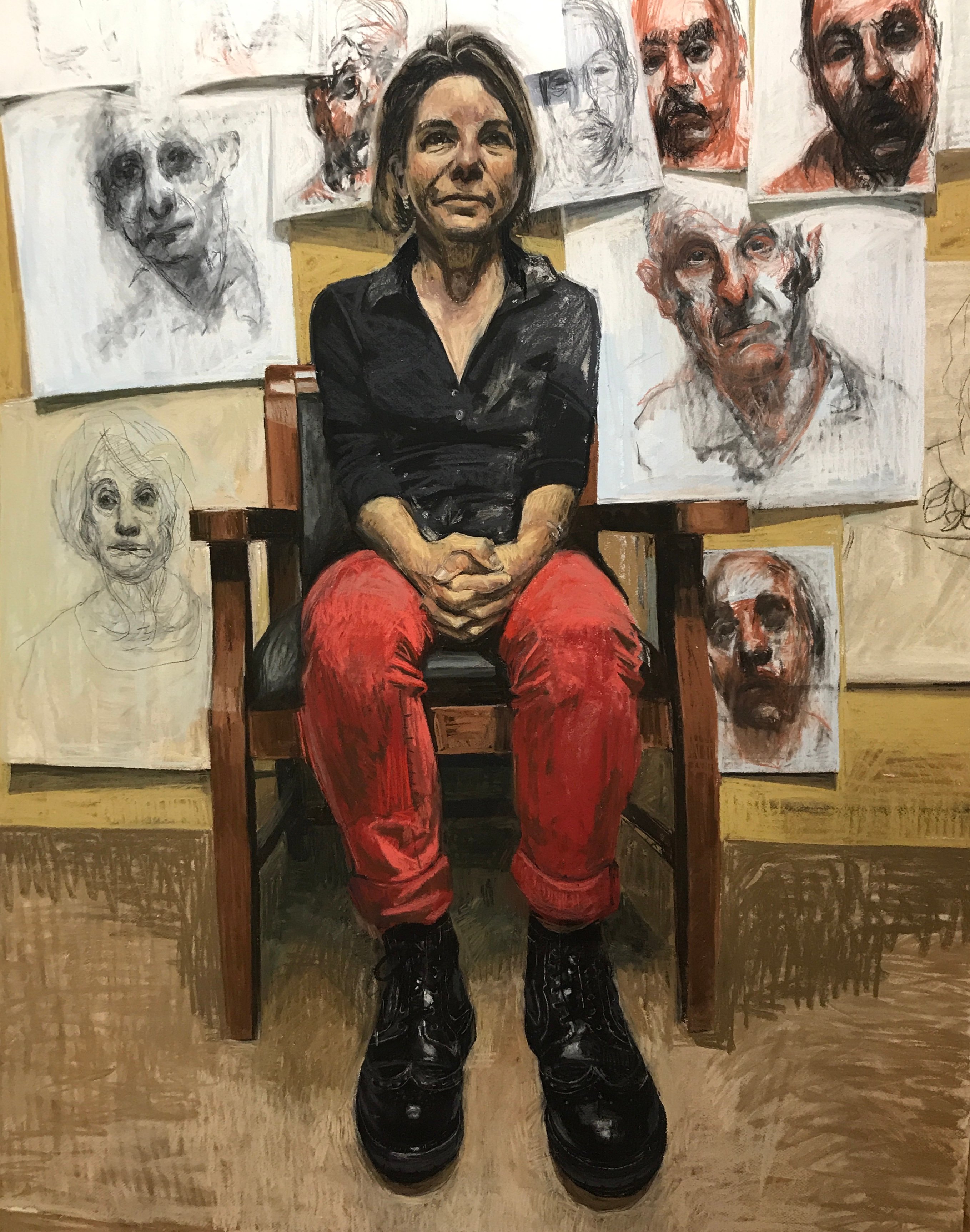
Courtesy of Mark Gilbert.
Pastel on paper.
Artists are thought to see the world differently than others because they can train their eye to focus on the details of the entire scene to reveal the person or object. They consider the white spaces and can break the image into a collection of lines, shadows, shapes, and contours. Dingfelder notes: “As a result, artists can paint pictures that jar regular people out of our well-worn habits of seeing.”16 Gilbert’s portraits of patients are the result of multiple sittings in different settings. In addition, he reviews photos and audio tapes of the sessions to capture the essence of the person and the person’s interaction with the caregiver. This way of seeing is similar to that of clinicians working with people living with dementia.
Health care professionals’ work with people living with dementia is like creating portraits of people. For, in order to make a diagnosis of dementia, the clinician must assess the person by comparing what is known about the person in the present and in the past, prior to the illness. The clinician interviews the person and the caregiver separately, taking careful inventory of the person’s loss of function in key areas and documenting changes in personality and behavior. Timelines are measured in intervals to determine if this loss of function is an acute medical problem or sign of a progressive illness. Further complicating the diagnostic process is the fact that two-thirds of people with dementia lack insight that they have the disease.17 Therefore, they often do not recognize they have a problem, and clinicians must rely on information about changes from people around them to make the diagnosis. People’s lack of awareness of memory deficits affecting their function becomes the number one hurtle to their forming a therapeutic relationship and accepting a supportive care plan. It is here where the art happens.
How do you convey to persons with memory loss and other cognitive impairments that they have a problem when they do not believe they do? How can you be seen as a trusted ally with their best interests at heart? Such persons must know and feel that you see them.
To best accomplish this goal of seeing people who are living with dementia, the clinician must face the responsibility and challenge of seeing them in their entirety, both present and past, at a time when their ability to recall and express who they are begins to fade. It is often the unspoken hurts and disappointments of lived experience that form the person seated before the clinician. A key to this process of seeing is teasing out a detailed social history of the person, which considers intimate relationships and social supports while also noting the person’s level of risk tolerance and how they adjust to change.
Because people with dementia are often older and frail and do not recognize or have insight into their deficits, a home visit by geriatricians and other health care professionals often provides a true picture of how they are dealing with their memory and functional issues. At home, a shift in the power dynamic makes the person with dementia a comfortable host. With environmental clues, the clinician can prompt the person to share more of the richness of their life story. The clinician can also observe details of the person’s daily life, such as what food is in the refrigerator, if the person takes their medication, and their ability to access their bathroom and bedroom.
The clinician then creates an assessment report—similar to a portrait—of the person with dementia that records their life story, values, and wishes while the person can still express them. When the clinician next sees the person, the person might be unable to remember having met the clinician and the last encounter, but the clinician certainly remembers the person.
Cox K. Brushes with the past. Globe and Mail. March 7, 2000. https://www.theglobeandmail.com/arts/brushes-with-the-past/article25457424/. Updated March 27, 2018. Accessed February 25, 2020.
Museum of Modern Art (MOMA). The artist is present. https://www.moma.org/learn/moma_learning/marina-abramovic-marina-abramovic-the-artist-is-present-2010/. Accessed April 3, 2020.
Fogh J. On seeing and being seen. Vital Voice Blog. https://vitalvoicetraining.com/blog/on-seeing-and-being-seen. Accessed April 3, 2020.
Perry VG, Wolburg JM. Aging gracefully: emerging issues for public policy and consumer welfare. J Consum Aff. 2011;365-371.
Brenoff A. Here’s the real reason older women don’t want to be invisible. AARP Stories. May 8, 2019. https://www.aarp.org/disrupt-aging/stories/info-2019/women-feeling-invisible.html. Accessed April 3, 2020.
Busch A. The invisibility of older women. Atlantic. February 27, 2019. https://www.theatlantic.com/entertainment/archive/2019/02/akiko-busch-mrs-dalloway-shows-aging-has-benefits/583480/. Accessed February 25, 2020.
Sheridan Centre for Elder Research; Revera. Revera report on ageism: independence and choice as we age. https://docisolation.prod.fire.glass/?guid=102a613b-8771-487d-6b5a-513f9f212d91. Published 2016. Accessed February 24, 2020.
Cations M, Radisic G, Crotty M, Laver KE. What does the general public understand about prevention and treatment of dementia? A systematic review of population-based surveys. PLoS One. 2018;13(4):e0196085.
Smyth W, Fielding E, Beattie E, et al. A survey-based study of knowledge of Alzheimer’s disease among health care staff. BMC Geriatr. 2013;13:2.
Dingfelder SF. How artists see. Monitor on Psychology. 2010;41(2):40.
Mace NL, Rabins PV. The 36-Hour Day: A Family Guide to Caring for People Who Have Alzheimer Disease, Related Dementias, and Memory Loss. Baltimore, MD: Johns Hopkins University Press; 1981.



