Case and Commentary
Oct 2024
Peer-Reviewed

Short sleep duration, poor sleep quality, and irregular timing of sleep are prevalent sleep troubles for children, but fully assessing children’s sleep environments and effectively promoting children’s overall sleep health is nearly impossible during brief clinical encounters. This commentary on a case suggests strategies for navigating this problem with a patient- and family-centered approach that prioritizes identifying family sleep-related beliefs, values, and goals and maintaining flexibility when offering evidence-based recommendations to improve children’s sleep.
LJ is a 12-year-old arriving with their parents to an appointment with Dr Z. LJ has been more distracted and disruptive in school, their grades have dropped from a B+ average to a C, and a teacher recently mentioned seeing them dozing during class. Dr Z speaks with LJ alone and learns that LJ’s father was recently laid off from a long-time job, prompting the family to sell their home and move to an apartment. LJ’s mother has taken on 2 new jobs and is often not home until 11:00 pm, past LJ’s bedtime, which is now much harder for LJ’s parents to enforce. LJ now plays video games late into the night, delaying sleep onset, and typically wakes up a few hours later due to noise from neighbors in an adjacent apartment or on the stairs. LJ’s mother can no longer drop them off at school, so LJ must be prompt to catch the school bus at 7:00 am. Most nights, LJ gets 5 to 6 hours of sleep. LJ also tells Dr Z, “My mom and dad aren’t very happy right now. I make things worse for them when I don’t do well in school.” LJ and their family have identified LJ’s daytime sleepiness and poor grades as top problems at this visit. Dr Z considers how to address these changes in LJ’s life and LJ’s shortened sleep duration with their parents.
Dr Z wonders how to recruit LJ’s parents as allies in protecting LJ’s sleep time and quality.
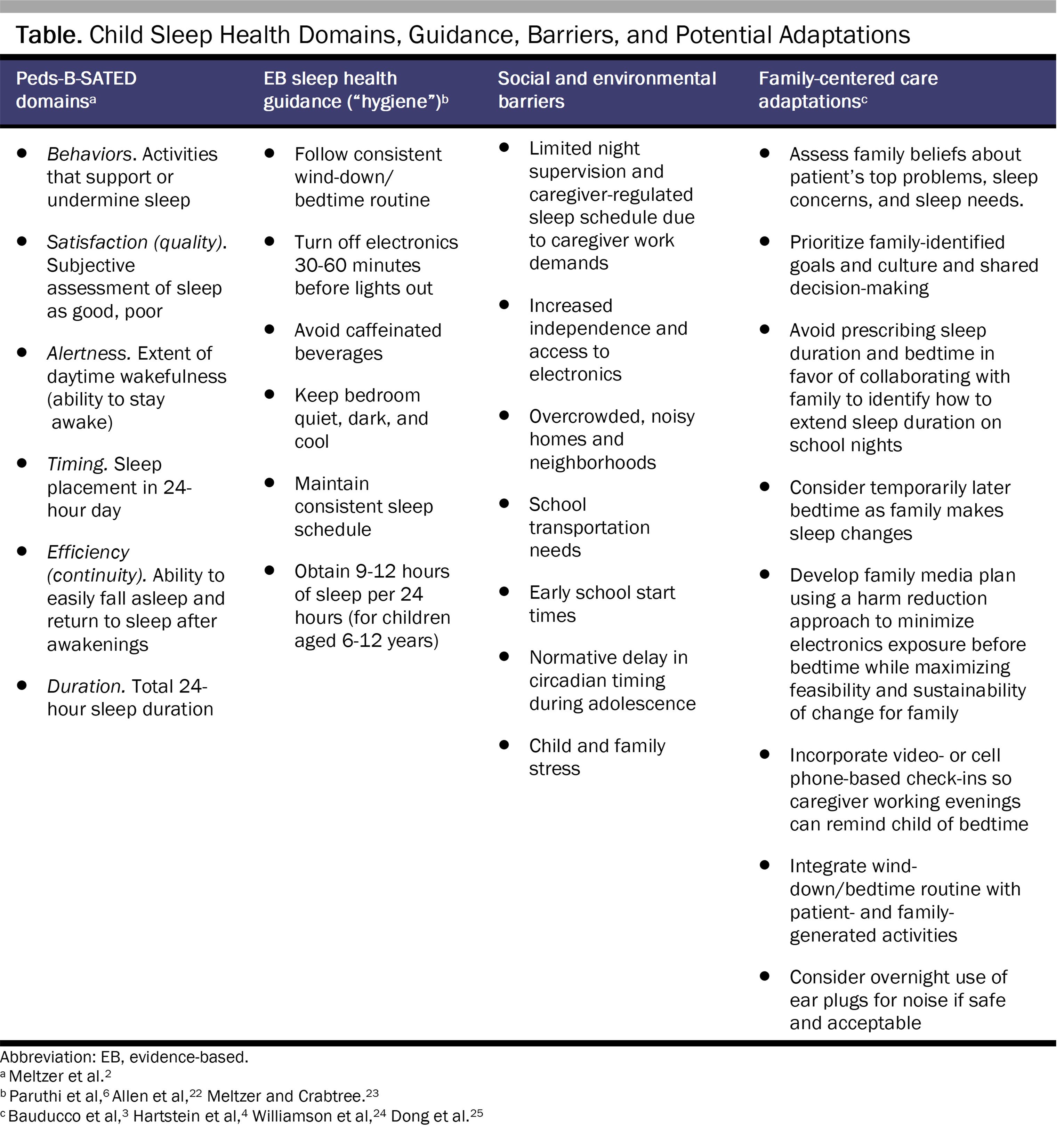
Child sleep health is multidimensional and determined by multiple factors. LJ’s case reflects how many social and environmental factors, including family transitions and related stress, caregiver work schedules, the home sleep environment, school start times, and the neighborhood context, can interact to produce poor pediatric sleep health.1,2 Importantly, pediatric sleep health comprises multiple domains that are represented by the Peds-B-SATED framework: pediatric sleep-related behaviors (eg, nighttime electronics usage), satisfaction (perceived sleep quality), alertness during the day, timing of sleep, efficiency of sleep (ie, continuity or awakenings), and sleep duration.2
LJ’s concerns cut across nearly all sleep health domains. LJ’s evening video gaming is a poor sleep health behavior that has led to a later bedtime and a prolonged sleep onset latency, as electronics usage before bedtime can increase stimulation and disrupt sleep.3,4 To assess satisfaction with and timing of sleep, Dr Z could ask LJ about their perceived sleep quality and sleep schedule during weekdays and on weekends, respectively.2 Night awakenings due to neighborhood noise reflect poor efficiency or continuity of sleep, likely contributing to daytime sleepiness (ie, diminished alertness).2 Further contributing to diminished alertness at school,5 LJ experiences insufficient sleep duration, as 5- to 6 hours is less than the 9-to-12-hour total sleep duration recommended for children aged 6 to 12 years.6
Sleep and child well-being are closely linked.7 There is robust evidence that short sleep duration in childhood is associated with worse academic performance, worse mental health, and increased risk of obesity and other cardiometabolic concerns.7 Especially relevant to LJ, experimental research shows that sleep-restricted youth are more likely to experience inattention, irritability, and emotional lability.8,9 Although less research is available on other aspects of sleep health, such as daytime sleepiness10 and irregular sleep timing,11 these aspects are similarly associated with adverse child outcomes, including mental health problems. Thus, poor sleep health likely contributes to LJ’s current academic and psychosocial difficulties. There is also evidence that poor sleep health could exacerbate the impacts of lower family socioeconomic status and related stressors on child cognitive and mental health functioning,12,13,14 making it even harder for LJ to cope with recent family changes. Given the link between poor child sleep and depressive symptoms and suicidality,15 Dr Z should also consider administering available child mental health screeners (eg, the Patient Health Questionnaire-9 item depression screener16) to identify whether the family could benefit from a mental health referral.
Ethically protecting child sleep time, sleep quality, and sleep health more broadly requires a patient- and family-centered approach,17 which is associated with increased patient and family care satisfaction and improved health care outcomes.18,19 Key principles of this approach include communication and collaboration with patients and families in health care planning and decision-making, recognizing and drawing upon patient and family strengths, and promoting health literacy.18,19 Simply providing LJ and their caregivers with sleep health recommendations, including age-based sleep duration guidance, prescribing an earlier bedtime, and removing video games, may feel impossible for the family, given the less modifiable factors contributing to LJ’s poor sleep (see Table). For instance, it is unlikely that LJ’s mother can change her work schedule. Moreover, removing electronics may be difficult if LJ uses video games to cope with family and school stress, distract from pre-sleep worry, or tune out neighborhood noise.20 Yet LJ cannot wake later in the morning to extend sleep duration since the family must rely on an early school bus for LJ’s transportation. LJ also may attend a middle school that starts earlier than the later times that better align with emerging preteen and adolescent social and circadian rhythms.5,21
To apply a patient- and family-centered approach, Dr Z should collaborate with LJ and their family to tailor evidence-based sleep recommendations22,23 to the family context, relevant social and environmental factors,24 and the family’s perspectives on LJ’s sleep.18,19 Ethically, minor patients like LJ should be involved in pediatric health care decision-making, with the physician taking a supportive role to encourage patient and family discussion while also respecting patient confidentiality.26 To promote health literacy as part of a patient- and family-centered approach, Dr Z could begin by providing psychoeducation about how poor sleep health may contribute to LJ’s current challenges using specific examples from the family’s report of LJ’s home and school functioning. Dr Z should emphasize the link between sleep and overall well-being and clearly communicate that improving sleep may benefit LJ’s functioning and help them cope with recent family stressors.27 In this discussion, normalizing the high rates of poor sleep health in children may facilitate a nonjudgmental interaction and help Dr Z join with LJ’s caregivers to promote healthier sleep. For example, Dr Z could share that more than 50% of middle school students do not obtain sufficient sleep on school nights28 and that many have trouble setting technology aside at bedtime.20
Positioning LJ and their parents as the experts on LJ’s sleep is crucial in joining with the family as an ally and generating feasible patient- and family-centered sleep health promotion strategies.24 Accordingly, Dr Z should directly ask LJ and LJ’s family about their sleep-related beliefs, goals, and any perceived barriers to healthy sleep.24 It could be that LJ believes engaging in video games helps distract them enough to fall asleep20 or that LJ or their parents do not feel LJ needs as much sleep as is recommended by national guidelines. Understanding these perspectives, along with family-identified goals and perceived barriers, can support subsequent collaboration18,19 in addressing LJ’s sleep. As shown in the Table, evidence-based sleep health guidance could be tailored to better align with the family context. Instead of prescribing a specific bedtime and sleep duration for LJ, Dr Z could work with the family to identify a bedtime—not too early in the evening—that would enable LJ to get the most sleep possible. Getting into bed too early could exacerbate LJ’s reported difficulty falling asleep, and it may be necessary to begin with a temporarily later bedtime (eg, 11:00 pm) that is gradually moved earlier as the family makes other sleep changes.23 Although LJ may be prepubertal, it could also be helpful to make the family aware that adolescents normatively experience a circadian delay with the onset of puberty, with a preference for later bedtime due to both biological and social factors (eg, increased independence, more social activities).21
To begin partnering with the family to address LJ’s sleep, Dr Z should collaborate with the family members to develop brief, tailored wind-down or bedtime routines that include reducing electronic device use and encouraging activities that reduce hyperarousal before bedtime.23,25 Dr Z should emphasize the importance of caregiver involvement in establishing bedtime routines and limiting screen time,3,29 while also acknowledging any identified family sleep-related beliefs, goals, and barriers. Rather than recommending that LJ avoid electronics altogether 30 to 60 minutes before bedtime,4 which may not be realistic for many youth, Dr Z could engage the family in collaborative problem-solving to set a patient- and family-identified video game and electronics stop time as part of a family media plan.29,30 The family and LJ could also set reminders on their cellular phones to turn the game off, initiate video check-ins before bedtime if the caregiver who is working can take a break,24 or enable parental controls to block internet access after a certain time each evening. Similar to patient- and family-centered care, collaboration and promotion of autonomy are core motivational interviewing principles.31,32 By using motivational interviewing approaches,25,31 such as exploring the advantages and disadvantages of reducing video game usage at night, Dr Z could help engage LJ in problem-solving and help facilitate positive change.32 Rather than eliminating evening electronics usage altogether, Dr Z and the family could develop a harm reduction approach consisting of incremental, sustainable reductions33 in video game usage. LJ could also earn video game time the next day if he is able to adhere to the family-identified school night bedtime.
Dr Z should also suggest that the wind-down or bedtime routine incorporate strategies for helping LJ cope with any low mood or negative self-referential thoughts concerning sleep, school performance, and family stress.25,27 Such strategies might include relaxation techniques and the development of coping thoughts (eg, I am working on my sleep to do better at school or this is a stressful time for my family, but it will get better) to replace negative thoughts reported by LJ during the visit. Throughout this discussion, Dr Z should continue to collaborate with both LJ and their caregivers to personalize these recommendations and address barriers to implementation.33 Finally, if it is acceptable to the family and safe for LJ, ear plugs could be used overnight to block out neighborhood noise. Using a sound machine or white noise cellular phone app, with the phone plugged in across the room or set face down to prevent usage, could also help to reduce sleep-interfering noises overnight. Collaborating with the family to finalize an agreed-upon sleep plan using importance and confidence rulers—another motivational interviewing strategy31,32—could help Dr Z assess each family member’s perceptions and facilitate behavior change.33
Developing a tailored plan to address poor pediatric sleep health can be challenging during a time-limited well-child or follow-up visit. Providing written sleep health education could increase clinical efficiency, but education is rarely sufficient for producing meaningful behavior change.34 More specifically, applying a one-size-fits-all approach to sleep guidance neglects the crucial social and environmental factors underlying sleep health disparities, which begin in childhood.1 Taking the time to position LJ and their family as experts and to engage them in generating personalized, feasible strategies to improve LJ’s sleep would likely yield greater patient and family benefits18,19 and could motivate subsequent behavior change.33 At the very least, a patient- and family-centered approach would help Dr Z join with the family as an ally and avoid contributing to the family’s already high level of social and environmental stress.
Meltzer LJ, Williamson AA, Mindell JA. Pediatric sleep health: it matters, and so does how we define it. Sleep Med Rev. 2021;57:101425.
Bauducco S, Pillion M, Bartel K, Reynolds C, Kahn M, Gradisar M. A bidirectional model of sleep and technology use: a theoretical review of how much, for whom, and which mechanisms. Sleep Med Rev. 2024;76:101933.
Au R, Carskadon M, Millman R, et al; Adolescent Sleep Working Group; Committee on Adolescence; Council on School Health. School start times for adolescents. Pediatrics. 2014;134(3):642-649.
Matricciani L, Paquet C, Galland B, Short M, Olds T. Children’s sleep and health: a meta-review. Sleep Med Rev. 2019;46:136-150.
Becker SP, Sidol CA, Van Dyk TR, Epstein JN, Beebe DW. Intraindividual variability of sleep/wake patterns in relation to child and adolescent functioning: a systematic review. Sleep Med Rev. 2017;34:94-121.
Goldstein TR, Franzen PL. Sleep difficulties and suicidality in youth: current research and future directions. Curr Opin Psychol. 2020;34:27-31.
American Medical Association. Opinion 2.2.1 Pediatric decision making. Code of Medical Ethics. Accessed August 30, 2024. https://code-medical-ethics.ama-assn.org/ethics-opinions/pediatric-decision-making
Committee on Hospital Care; Institute for Patient- and Family-Centered Care. Patient- and family-centered care and the pediatrician’s role. Pediatrics. 2012;129(2):394-404.
Daniels A, Pillion M, Rullo B, et al. Technology use as a sleep-onset aid: are adolescents using apps to distract themselves from negative thoughts? Sleep Adv. 2022;4(1):zpac047.
Allen SL, Howlett MD, Coulombe JA, Corkum PV. ABCs of sleeping: a review of the evidence behind pediatric sleep practice recommendations. Sleep Med Rev. 2016;29:1-14.
Meltzer LJ, Crabtree VM. Pediatric Sleep Problems: A Clinician’s Guide to Behavioral Interventions. American Psychological Association; 2015.
American Medical Association. Opinion 2.2.2 Confidential health care for minors. Code of Medical Ethics. Accessed July 1, 2024. https://code-medical-ethics.ama-assn.org/ethics-opinions/confidential-health-care-minors
American Academy of Pediatrics. Make a family media plan. HealthyChildren.org. Accessed July 1, 2024. https://www.healthychildren.org/English/family-life/Media/Pages/How-to-Make-a-Family-Media-Use-Plan.aspx
Rollnick S, Miller WR. What is motivational interviewing? Behav Cogn Psychother. 1995;23(4):325-334.
Gold MA, Kokotailo PK. Motivational interviewing strategies to facilitate adolescent behavior change. American Academy of Pediatrics; 2007. Accessed September 18, 2024. https://www.scribd.com/document/742976406/Motivational-Interviewing-Strategies-to-Facilitate-Adolescent-Behavior-Change
Quante M, Khandpur N, Kontos EZ, Bakker JP, Owens JA, Redline S. “Let’s talk about sleep”: a qualitative examination of levers for promoting healthy sleep among sleep-deprived vulnerable adolescents. Sleep Med. 2019;60:81-88.



