Medicine and Society
Jun 2024
Peer-Reviewed

Despite growth in numbers of organizational antimicrobial stewardship programs, antimicrobial resistance continues to escalate. Interprofessional education and collaboration are needed to make these programs appropriately responsive to the ethically and clinically complex needs of patients at the end of life whose care plans still require antimicrobial management.
More than 2.8 million antimicrobial-resistant infections and 35 000 deaths from antibiotic resistance are reported to occur annually.1 Escalating rates of antimicrobial resistance have called attention to the need for antimicrobial stewardship programs and infection control measures.2,3,4 Although antimicrobial misuse is a problem across the lifespan, overtreatment with antibacterials is common at the end of life.5 The proportion of end-of-life or comfort-care patients receiving an antimicrobial has been estimated to be as high as 77%,6,7,8 yet only 15% meet criteria for antimicrobial treatment.9 In particular, nonbeneficial antimicrobial therapy is provided to a substantial number of end-of-life patients with advanced stage cancer,10 with advanced dementia,11 and who are on comfort-care protocols.6,9,12,13 Despite implementation of antimicrobial stewardship programs,14 prescribing and using antimicrobials for individuals at the end of life is complicated by a number of ethics questions that affect all of us.15 Failure to identify key features of antimicrobial misuse results in ineffective treatments, more multidrug-resistant organisms, prolonged suffering, and increased systemic burden.5,16
Recent research on antimicrobial use at the end of life has focused on prescribing patterns and factors contributing to them rather than generating evidence-based interventions.6,7,10,17,18,19 Antimicrobial drug overuse and misuse often result from clinicians’ inadequate education about antimicrobial drug stewardship,20 tendencies to treat symptoms rather than identified microorganisms,21 and yielding to patients’ and families’ non-evidence-based desires for treatment.18,22 Antimicrobial treatments at the end of life persist despite the fact that they are often ineffective, do not alleviate symptoms,7,8 and do not result in a significant increase in the quality or length of life.23
It is imperative to implement systems to overcome these challenges. Some tool kits have resulted in more responsible antimicrobial use, but it is unknown whether those changes are sustainable.8,24 Recent increases in rates of antimicrobial resistance25 suggest that the tool kits have not curbed resistance. In addition, recent changes to the nurse, physician, and pharmacy workforces as a result of the COVID-19 pandemic could have undermined previous work on antimicrobial stewardship and antimicrobial resistance.26,27,28,29,30
Antimicrobial stewardship can improve effectiveness in treatment of infectious diseases and protect against the harm associated with antimicrobial misuse in the care of patients, especially those at end of life. However, limiting antimicrobial use can present an ethical dilemma for some clinicians. Because clinicians work closely with patients, they are often morally and emotionally compelled to focus on patients’ individual rights and well-being rather than on the well-being of the public as a whole.
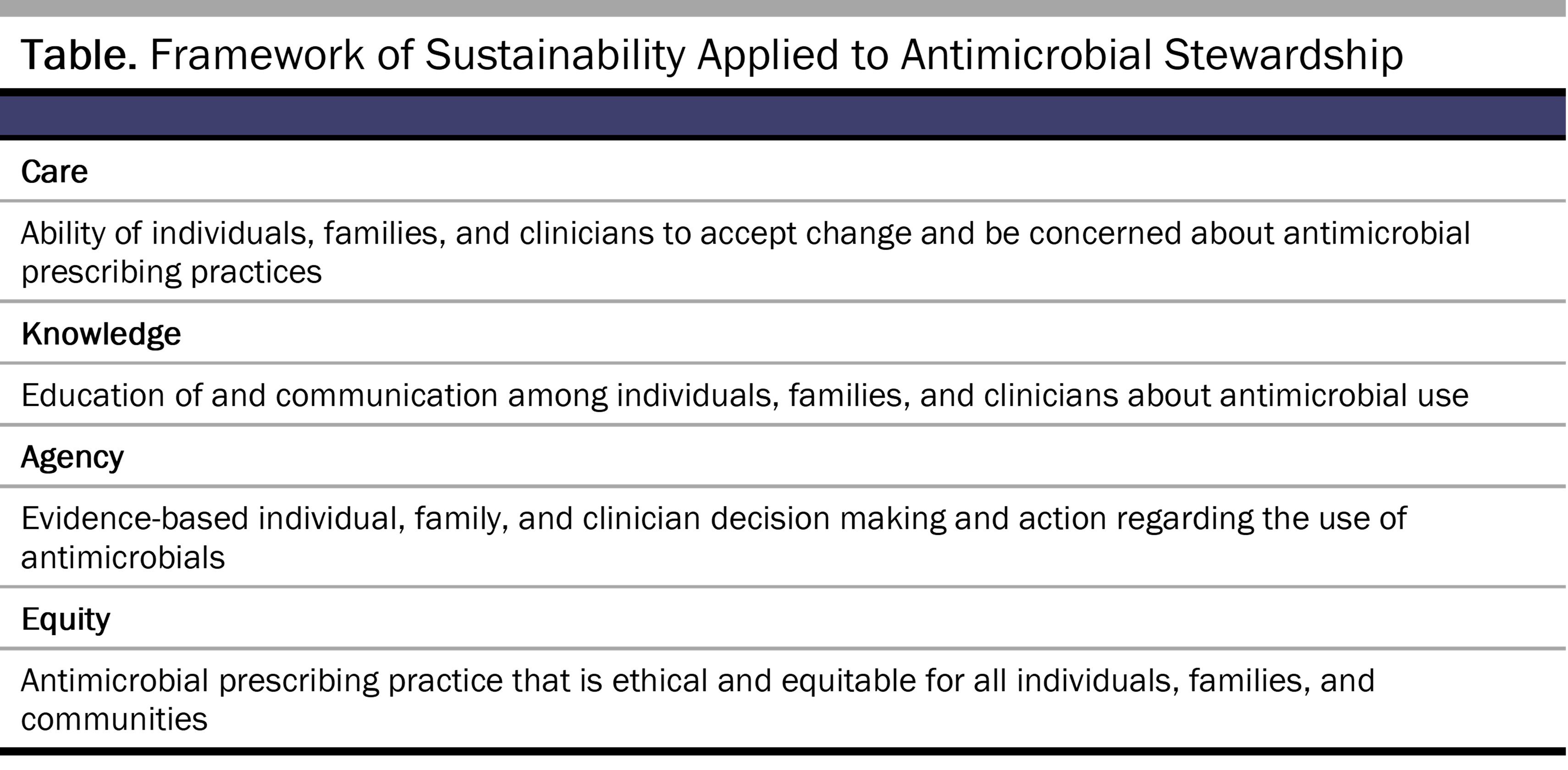
This tension between helping one and helping many agents is a common one in public health ethics, particularly in individualistic societies, and addressing this tension in end-of-life care requires a shift from serving individuals (an autonomy focus) toward serving the collective (an equity focus) to achieve the goals of stewardship.31 Theoretical work in environmental sciences has explored the importance of care and relational values, which reflect the centrality of the collective in fostering stewardship.32,33 Building on a framework with 3 elements of stewardship—care, knowledge, and agency32 we propose a framework of sustainability that adds a fourth element—equity—which could have utility in the promotion of antimicrobial stewardship (see Table). Care, as a normative and subjective element of the framework, is necessary because it motivates an individual to attend to, or care about, an issue such as antimicrobial resistance and its impact on humanity. Knowledge, another core element of stewardship actions, may currently be inadequate to combat antimicrobial resistance,20 making education for clinicians and the public critical to the promotion of stewardship.34 Agency, the third element of the framework, denotes the capacity of people to affect change, particularly through collective action. Equity, as applied to end-of-life care, highlights the ambiguity inherent in medicine and the need for not only a forthright discussion of what it means for patients to be at the end of their lives, but also potential consideration of the impact of antimicrobial use on antimicrobial resistance. The misuse of antimicrobials at the end of life is not easily combatted by individuals alone but instead will require a collective approach regarding common practices and expectations for the end of life that are equitable. Care, knowledge, and agency are intertwined.33 Adding an explicit discussion of equity rather than a focus on autonomy makes all these framework elements necessary to advance stewardship.
Despite a desire to have discussions with their clinicians about end-of-life care, many patients do not engage in these discussions.35 Patients who are at risk for a life-threatening clinical event due to a serious life-limiting medical condition can benefit from advance care planning, such as by completing the Physician Orders for Life Sustaining Treatment.36 However, focusing on documents may undermine efforts to engage in meaningful conversations about advance care planning for patients nearing the end of their lives.37 There is consensus that comprehensive advance care planning should include intentional discussion about infection management.20 If a patient’s goals are comfort at the end of life, antimicrobial use may unnecessarily complicate achieving those goals.38,39
Use of antimicrobials has become ubiquitous in modern medicine—so much so that patients often expect and pressure physicians to prescribe antimicrobials even when they are not indicated.40 Acquiescing to patients’ requests for antimicrobials when they are not medically indicated illustrates an overemphasis on patient autonomy. An equitable approach to antimicrobial stewardship should redirect the focus from respect for autonomy to that of the common good. However, inconsistent information on antimicrobial effectiveness for treating symptoms or prolonging life8,41 contributes to the challenges of establishing ethical and equitable antimicrobial use for patients who likely are facing the end of life. Given that the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America identify antibiotic therapy as aggressive care at the end of life,42 it’s potentially inappropriate if it cannot achieve the intended goals of care.43 Rather than focus on individual preferences about specific treatment options, physicians should consider using an algorithm5 or a decision support aid when considering antimicrobial use in end-of-life situations.24 Treating an infection as part of end-of-life care could delay a shift to a more comfort-focused plan of care and thus contribute to additional suffering of a patient who may survive the infection only to experience additional discomfort from the underlying disease process.5
Minimizing long-term harms of antimicrobial resistance requires a rapid coordinated response, including the mounting of rigorous surveillance systems to monitor antimicrobial resistance patterns, implementation of antimicrobial drug stewardship protocols aimed at decreasing the overuse and misuse of antimicrobials, and scaling up of quality infection prevention and control systems.17,44 The US National Action Plan for Combating Antibiotic-Resistant Bacteria, 2020-2025, stresses that evidence-based interventions are essential to control antimicrobial resistance and combat its sequelae.45
Further work is needed to (1) assess the effect of antimicrobial stewardship protocols on antimicrobial use at the end of life, (2) analyze the impact of antimicrobial use on symptom management, (3) explore quality-of-life implications of antimicrobial use, (4) develop decision support tools to advance informed ethical decisions about antimicrobial use at the end of life, (5) standardize clinician education on antimicrobial stewardship and ethical considerations at the end of life, and (6) implement ethical and equitable standards for end-of-life care that could inform future antimicrobial stewardship programs.
Centers for Disease Control and Prevention. Antibiotic Resistance Threats in the United States, 2019. US Department of Health and Human Services; 2019. Accessed January 10, 2023. https://www.cdc.gov/drugresistance/pdf/threats-report/2019-ar-threats-report-508.pdf
Centers for Disease Control and Prevention. COVID-19: US impact on antimicrobial resistance, special report 2022. US Department of Health and Human Services; 2022. Accessed January 19, 2024. https://stacks.cdc.gov/view/cdc/119025/cdc_119025_DS1.pdf?download-document-submit=Download
Furuno JP, Noble BN, Fromme EK. Should we refrain from antibiotic use in hospice patients? Expert Rev Anti Infect Ther. 2016;14(3):277-280.
Emberger J, Tassone D, Stevens MP, Markley JD. The current state of antimicrobial stewardship: challenges, successes, and future directions. Curr Infect Dis Rep. 2018;20(9):31.
World Bank Group. Drug-Resistant Infections: A Threat to Our Economic Future. International Bank for Reconstruction and Development; 2017. Accessed June 20, 2023. https://documents1.worldbank.org/curated/en/323311493396993758/pdf/final-report.pdf
Larnard J, Blackshear L, Lee MSL, Buss MK, Stead W. Perceptions and reality of antimicrobial prescribing during the transition to comfort measures only at an academic medical center. Open Forum Infect Dis. 2022;10(1):ofac692.
Datta R, Topal J, McManus D, Dembry LM, Quagliarello V, Juthani-Mehta M; SHEA Research Network. Perspectives on antimicrobial use at the end of life among antibiotic stewardship programs: a survey of the Society for Healthcare Epidemiology of America Research Network. Infect Control Hosp Epidemiol. 2019;40(9):1074-1076.
Eremin S, Escher M, Ivanovska V, et al. Global Antimicrobial Resistance and Use Surveillance System (GLASS) report 2022. World Health Organization; 2022. Accessed January 19, 2024. https://iris.who.int/bitstream/handle/10665/364996/9789240062702-eng.pdf?sequence=1
Leber AL, Peterson E, Dien Bard J; Personnel Standards and Workforce Subcommittee, American Society for Microbiology. The hidden crisis in the times of COVID-19: critical shortages of medical laboratory professionals in clinical microbiology. J Clin Microbiol. 2022;60(8):e0024122.
Enqvist JP, West S, Masterson VA, Haider LJ, Svedin U, Tengö M. Stewardship as a boundary object for sustainability research: linking care, knowledge and agency. Landsc Urban Plan. 2018;179:17-37.
West S, Haider LJ, Masterson V, Enqvist JP, Svedin U, Tengö M. Stewardship, care and relational values. Curr Opin Environ Sustain. 2018;35:30-38.
Michael CA, Dominey-Howes D, Labbate M. The antimicrobial resistance crisis: causes, consequences, and management. Front Public Health. 2014;2:145.
Strumiło J, Chlabicz S, Pytel-Krolczuk B, Marcinowicz L, Rogowska-Szadkowska D, Milewska AJ. Combined assessment of clinical and patient factors on doctors’ decisions to prescribe antibiotics. BMC Fam Pract. 2016;17(1):63.
Fairweather J, Cooper L, Sneddon J, Seaton RA. Antimicrobial use at the end of life: a scoping review. BMJ Support Palliat Care. Published online November 30, 2020.
Bosslet GT, Pope TM, Rubenfeld GD, et al; American Thoracic Society ad hoc Committee on Futile and Potentially Inappropriate Treatment; American Thoracic Society; American Association for Critical Care Nurses; American College of Chest Physicians; European Society for Intensive Care Medicine; Society of Critical Care. An official ATS/AACN/ACCP/ESICM/SCCM policy statement: responding to requests for potentially inappropriate treatments in intensive care units. Am J Respir Crit Care Med. 2015;191(11):1318-1330.
Tracking antimicrobial resistance. Centers for Disease Control and Prevention. November 23, 2021. Accessed June 26, 2023. https://www.cdc.gov/drugresistance/tracking.html#anchor_1630094068257
Office of the Assistant Secretary for Planning and Evaluation. National Action Plan for Combating Antibiotic-Resistant Bacteria, 2020-2025. US Department of Health and Human Services; 2020. Accessed June 20, 2023. https://aspe.hhs.gov/sites/default/files/migrated_legacy_files//196436/CARB-National-Action-Plan-2020-2025.pdf



