Medical Education
Jan 2023
Peer-Reviewed

US health care is segregated by insurance status and de facto by race; however, traditional models of medical education do not teach students about segregated care, and the authors know of no examples in the literature problematizing segregated care in medical education. To fill this gap, this article describes a student-led effort to disseminate peer-to-peer segregated care education at a single-site, large academic health system in New York City. It also provides educational resources that other student-advocates can adopt to drive curricular inclusion efforts at their own institutions. This article concludes that the primary goal of advocacy to teach segregated care is always desegregation, so curricular inclusion efforts are needed to educate students about the inequitable systems they are entering and to provide them with tools to advocate against such systems.
Segregation has long been the mechanism through which access to societal resources is limited by race. Structural segregation—the racialized mechanism through which Black Americans are denied equitable access to social goods, including housing, employment, and medical care—persists, despite civil rights legislation outlawing it. In this article, we are concerned with segregation within health care, termed segregated care, which, as noted in the 1990s,1,2,3 and as continues to be noted in the present day,4 manifests as race-based disparities in health outcomes and in access to clinics, physicians, dentists, and pharmacies.
Segregated care also manifests as health insurance inequities. In New York State, nonelderly Black adults are more likely to be enrolled in Medicaid and more likely to be uninsured than their White counterparts.5,6,7 Furthermore, public insurance eligibility restrictions—including for undocumented patients, for patients with incomes less than 50% of the federal poverty level, and for adult patients without dependent children—restrict Black Americans from coverage at nearly 2 times the rate of White Americans.6 While insurance status is fluid, the available statistics clearly demonstrate that segregating care by insurance status is de facto racial segregation.
Among our ethical responsibilities as medical professionals is to ensure justice in the allocation of medical resources, which requires “nonjudgmental regard and equal treatment for all with similar medical needs.”8 While individual clinicians might give the same care to all of their patients, insurance that segregates patients by race, class, and associated proxy markers results in unequal treatment.
Accordingly, this article seeks (1) to describe a student-led effort to disseminate peer-to-peer education about segregated care at a large academic health system in New York City and (2) to provide resources to other student-advocates and medical school administrators looking to educate their students about segregated care.
In 2014, Icahn School of Medicine at Mount Sinai (ISMMS) medical students founded the Segregated Care Student Workgroup in order to critically investigate segregated care in both outpatient and inpatient settings across the Mount Sinai Health System. As in many academic medical centers, patients with Medicaid were often seen in resident-run clinics, while patients with private insurance were often seen in separate, faculty-run clinics. Through a “secret shopper” study design, ISMMS medical students used a standard script to investigate differences in appointment wait times, one example of differences in care across sites. The study found that callers with Medicaid waited on hold significantly longer to make an appointment (9.8 minutes vs 1.3 minutes on average) and waited significantly longer for a scheduled appointment (13.4 days vs 54.3 days on average) (C. Braschi & L. Ostrer, unpublished data, 2015).
Student-led segregated care work at ISMMS has continued to grow over time. Students interviewed department heads and examined patient satisfaction data in relation to insurance status. Since 2018, student-leaders, including the 4 student authors (L.C., T.M.H., R.S., A.T.), have approached dismantling segregated care through medical education, hypothesizing that training students in a segregated system normalizes the practice and implicitly perpetuates racism. This commitment is particularly important because, as of mid-February 2022, we found no examples of teaching segregated care in medical education in the literature: a PubMed search for segregated care in the title or abstract—across all years and data sources—yielded only 9 results, none of which were about medical trainee education or curriculum development.
Since the group’s inception, members of the ISMMS Segregated Care Student Workgroup have provided extracurricular peer-to-peer segregated care education. In early 2020, student-leaders started seeking avenues through which to provide this education as part of the formal medical school curriculum to ensure that it reached all medical students, thereby eliminating the self-selection that often characterizes social justice advocacy.
Throughout 2020, student-leaders, who had built their expertise through involvement in past segregated care research and advocacy, designed and administered a peer-to-peer curricular and extracurricular education model. They generated presentation content and solicited input from expert faculty working at the intersection of racism, bias, and medicine. All presentations included introductory slides defining segregated care and contextualizing it within New York City (NYC) and the Mount Sinai Health System. This contextualization included quantitative data detailing the percentage of patients by insurance status and race nationally, in NYC, and within the Mount Sinai Health System. All presentations also included quantitative survey data from ISMMS students and residents about their observations of segregated care in clinical spaces and its impact on both care delivery and their perceptions of the health care system. Following the presentations, each session included discussion questions tailored to the audience’s particular curricular context—medical student, resident, attending physician, ancillary staff, or all health system staff—to generate further engagement with the material and to identify follow-up action items for students in the audience. A comprehensive list of educational opportunities provided throughout the year is outlined in the Table.
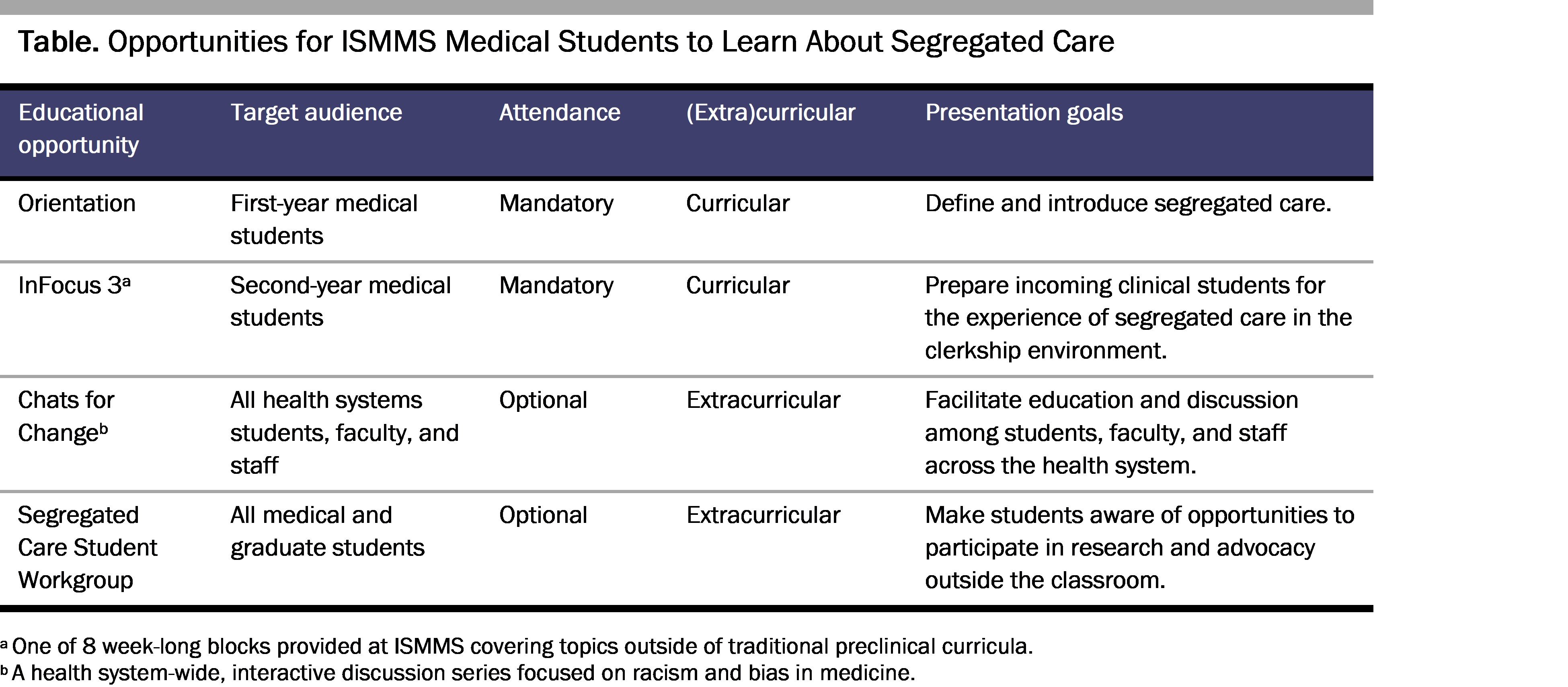
Orientation. Student-leaders created and administered a 10-minute peer-to-peer presentation during orientation for first-year medical students. Before their first day of medical school, incoming students learned about segregated care in a session asking them to examine the intersection of their social identities, their roles as medical students, and the health care system. Furthermore, the presentation sought to introduce the Segregated Care Student Workgroup and peer mentors to interested students. (Presentation slides are provided in Supplementary Appendix 1.)
InFocus 3. Student-leaders created and administered another 10-minute peer-to-peer presentation for second-year medical students during InFocus 3.9 The presentation focused on providing students the tools to recognize and question segregated care that they would likely experience during their upcoming third-year clerkships, elaborating on action items to guide student engagement. These action items asked students to “identify attending, fellow, and resident clinical role models that are challenging the status quo” and to “reflect on how experiencing segregated care in the clinical environment is impacting your education and personal well-being.” (Presentation slides are provided in Supplementary Appendix 2.) Following this session, presenting students informally collected feedback from attendees with the goal of improving the presentation year-over-year and further tailoring it to students entering the clinical environment. Open-ended prompts solicited students’ feedback on what they learned and what could be improved. (The feedback form is provided in Supplementary Appendix 3.)
Chats for Change. Outside the formal curriculum, student-leaders also designed and facilitated a 1-hour optional discussion open to all health system students, faculty, administrators, and staff. The presentation was part of the ISMMS Department of Medical Education’s Chats for Change.10 The presentation titled “Desegregating Care: Thinking Globally, Acting Locally” created a space for open dialogue about actions that individuals could take to challenge systemic and institutional segregated care. Discussion questions included the following: “What is the relationship between segregated care and racism?” and “What are the implications of working/practicing/teaching in a segregated system?” (The presentation, including discussion questions and action items, is provided in Supplementary Appendix 4.)
Mandatory education on segregated care for first- and second-year medical students, with additional extracurricular opportunities for those students interested in learning more, laid the foundation for these students to graduate with the ability to recognize segregated care, articulate its inequities, and implement skills to advocate for desegregation. However, these efforts had numerous shortcomings.
To begin addressing these shortcomings, student-leaders met privately with ISMMS administrators in January 2021 to facilitate a conversation about the inclusion of segregated care education into the formal curriculum. The meeting’s goals were to review student-led curricular inclusion efforts completed to date, to hear student-proposed ideas for longitudinal and institution-driven curricular inclusion, and to discuss the feasibility of these proposals from the administrators’ perspective. The proposed inclusion strategies involved adding discussions, case-based scenarios, and didactics within the framework of existing curricula. (See Supplementary Appendix 5 for the PowerPoint slides guiding this discussion.)
In this meeting, student-leaders received feedback and encouragement to create a written proposal outlining their vision. Administrators encouraged student-leaders to create a roadmap for curricular inclusion across all 4 years of medical school, to create specific curricular objectives, and to pair each objective with metric(s) to assess student mastery. The roadmap comprehensively integrates segregated care into existing sessions on racism and bias, clinical skills, and ethics in accordance with ISMMS’ Medical Education Program Objectives.11 For example, one suggestion involves modifying a session describing minority stress to include how segregation by insurance status could affect minority stress. During the live patient presentations included across preclinical courses, student-leaders suggested “actively and intentionally includ[ing] patients’ insurance status and other examples of racism/bias into patient presentations” (see Supplementary Appendix 6). Many more specific suggestions are included in the full proposal submitted to ISMMS administration and are provided in Supplementary Appendix 6. At the meeting, student-leaders received a verbal commitment that administrators would incorporate their recommendations in ongoing curricular efforts to strengthen antiracist medical education. Student-leaders and advocates continue to eagerly await institution-led efforts.
Macintyre S, Maciver S, Sooman A. Area, class and health: should we be focusing on places or people? J Soc Policy. 1993;22(2):213-234.
National Center for Health Statistics. Excess deaths and other mortality measures for the black population: 1979-81 and 1991. US Public Health Service; 1994.
Wilkinson R, Huxley-Reicher Z, Fox GC, et al. Leveraging clerkship experiences to address segregated care: a survey-based approach to student-led advocacy. Teach Learn Med. Published online June 30, 2022.
Uninsured rates for the nonelderly by race/ethnicity: 2019. Kaiser Family Foundation. Accessed February 25, 2022. https://www.kff.org/uninsured/state-indicator/nonelderly-uninsured-rate-by-raceethnicity/
Hill L, Artiga S, Orgera K, Damico A. Health coverage by race and ethnicity, 2010-2019. Kaiser Family Foundation. July 16, 2021. Accessed February 25, 2022. https://www.kff.org/racial-equity-and-health-policy/issue-brief/health-coverage-by-race-and-ethnicity/
Medicaid coverage rates for the nonelderly by race/ethnicity: 2019. Kaiser Family Foundation. Accessed August 3, 2022. https://www.kff.org/medicaid/state-indicator/nonelderly-medicaid-rate-by-raceethnicity/?currentTimeframe=0&sortModel=%7B%22colId%22:%22Location%22,%22sort%22:%22asc%22%7D
Rhodes R. Medical ethics: common or uncommon morality? Camb Q Healthc Ethics. 2020;29(3):404-420.
Second year. Icahn School of Medicine at Mount Sinai. Accessed February 25, 2022. https://icahn.mssm.edu/education/medical/program/year-two
What’s Chats for Change? Change Now, Icahn School of Medicine at Mount Sinai. April 2, 2021. Accessed February 25, 2022. https://changenow.icahn.mssm.edu/whats-chats-for-change/
Program curriculum. Icahn School of Medicine at Mount Sinai. Accessed August 10, 2022. https://icahn.mssm.edu/education/medical/program



