Medical Education
Jun 2020

Medical and especially surgical teaching stresses the importance of careful observation, developing tolerance for ambiguity, and cultivating empathy for patients’ and colleagues’ experiences of receiving and giving health care. Portraiture is defined by portraitist Mark Gilbert as a collaborative process between subject and artist; sitting is as critical to this process as painting or drawing. This article draws upon the second author’s work with Gilbert to examine how portraiture can motivate key teaching and learning goals in health professions education by facilitating learners’ explorations of their own and others’ biases, limitations, and approaches to gathering information from and about a source (eg, a subject or a patient).
In an operating room, the rest of the world falls away. Minor details are magnified when a patient’s life is in stasis, and each subtle variation in hue and texture can have significance. In this rarified space, it is a physician’s duty to notice clinically, ethically, and aesthetically relevant tactile and visual details from a full range of visual cues in the sterile field and drape of a surgical site and to interpret them in ways that create a foundation for good decision making in real time. The muted sheen of a patient’s superfluous fascia contrasts poorly with the thin lucency of that patient’s distal nerve; the consequences of a surgeon’s misjudgment about where to place a scalpel become magnified and intensified. Ideally, an experienced physician would have encountered this situation before and developed strategies for discerning color contrast among nerves and other tissues. Infinite variability persists, however, so it is impossible to offer a new physician in training a sufficient number of examples to lay the groundwork for confident, competent, and decisive action to proceed with an operation. Thus, curricula must nourish trainees’ cultivation of perception and their capacity to notice—and skillfully interpret the meaning of—the most relevant among a vast array of compelling details under conditions of uncertainty. Responding carefully and competently to uncertainty is a key and meaningful part of the art of medicine, and those who practice medicine—like those who practice visual arts—benefit from a diverse range of perceptual training experiences. In this article, we promote the value of this modality of training and provide examples of portraiture’s uses in health professions teaching and learning.
Portraiture, like medicine, incorporates specific and concrete characteristics and imbues them with contextual depth. In viewing either a body intraoperatively or a painting, an observer is forced to confront not only ambiguous details obscured by pooled blood or smears of paint, but also multiple decisions they might have made that contribute to the view before them. Surgeons and artists both create outcomes built upon a base coat of prior choices. A surgeon commits to a plane of dissection that can have permanent consequences for a patient; a portrait artist chooses a perspective that renders indelible the orientation of a subject on a canvas. Final form is shaped by choice and action, and both portrait artists—with brush or medium—and surgical trainees— with a hemostat or cautery—must be able to conceive a realm of possibilities, adumbrate their consequences, and then choose among and commit to actions.
Lest the comparison end at the operating room door, relentless attention to detail must guide every interaction in which a physician presumes to manage another’s life. By being trained with portraiture, learners can practice discernment skills before being called upon to serve the warm and breathing person who visits them in clinic.
Just as a clinician and a patient face each other in a clinical encounter, so a portrait artist and subject face each other in a sitting. Separating an artist and subject is a canvas on which an artist’s marks express that artist’s interpretation of a subject at a point in time; the canvas records the artist-subject relationship, influenced by the thoughts, personalities, and biases of both artist and subject. The portrait artist Mark Gilbert, with whom the second author worked on the Portraits of Care project,1 hopes the canvas justly and accurately represents a subject’s place on his or her journey during the time the two of them spent together doing portraiture (see Figure 1).
Figure 1. Jim With Radiotherapy Mask, by Mark Gilbert, 2014

Courtesy of Mark Gilbert.
Pastel on paper, 40" by 26".
If an artist is tempted to create a “pretty” portrait, biases that shape his or her conception of what constitutes pretty will likely generate inaccuracy—and possibly unjust inaccuracy. Just as a portrait artist must guard against bias, so must a clinician guard against jumping to a diagnosis and then retrofitting observations to confirm an erroneous first impression. Clinicians can avoid this trap by cultivating the capacity to recognize how their own biases from prior experiences, prejudices about people with backgrounds that differ from their own, and tendency to neglect the real-world prevalence of occurrences (ie, base-rate neglect) influence their thinking, reasoning, and decision making. They must learn to observe themselves and to interrogate information sources about patients, such as history, physical examination, laboratory results, and radiographic findings, each of which must be carefully weighed to yield knowledge that informs medical decisions that help patients. Learning to observe oneself as a clinician in these ways can be practiced with portraiture.
A portrait is a physical manifestation of an artist with a subject (who is often but not always sitting); it is one model of a patient-clinician relationship and thus is a useful tool for training clinicians. Portraits provide a snapshot of a subject at one point in time with variations and nuances that are apparent to some viewers but hidden to others. Through engaging with portraiture, learners can practice navigating uncertainty and assuming a variety of perspectives, for example. A portrait of a subject can accomodate a variety of interpretations; learners can practice orienting themselves not only to a plurality of perspectives on the subject’s experience that might initially make them uncomfortable, but also to the experiences, backgrounds, and moods of different viewers of the same subject. Metacognition can take place when learners witness and process their biases and thought patterns, share them with colleagues, and participate in team-based distributed cognition, all while practicing collegiality. Educators can also prime learners with phrases that subconsciously prompt them to see a portrait differently.
The canvas records the artist-subject relationship, influenced by the thoughts, personalities, and biases of both artist and subject.
For example, Mark Gilbert’s portrait, Henry De L, from the Saving Faces: Art and Medicine exhibit,2 can motivate students’ and trainees’ explorations of their emotional responses to a portrait (see Figure 2). Questions can include these: How does disfigurement influence your perception of Henry? What do you think you can say you know about him from how this portrait represents him?
Figure 2. Henry De L, by Mark Gilbert, 1999
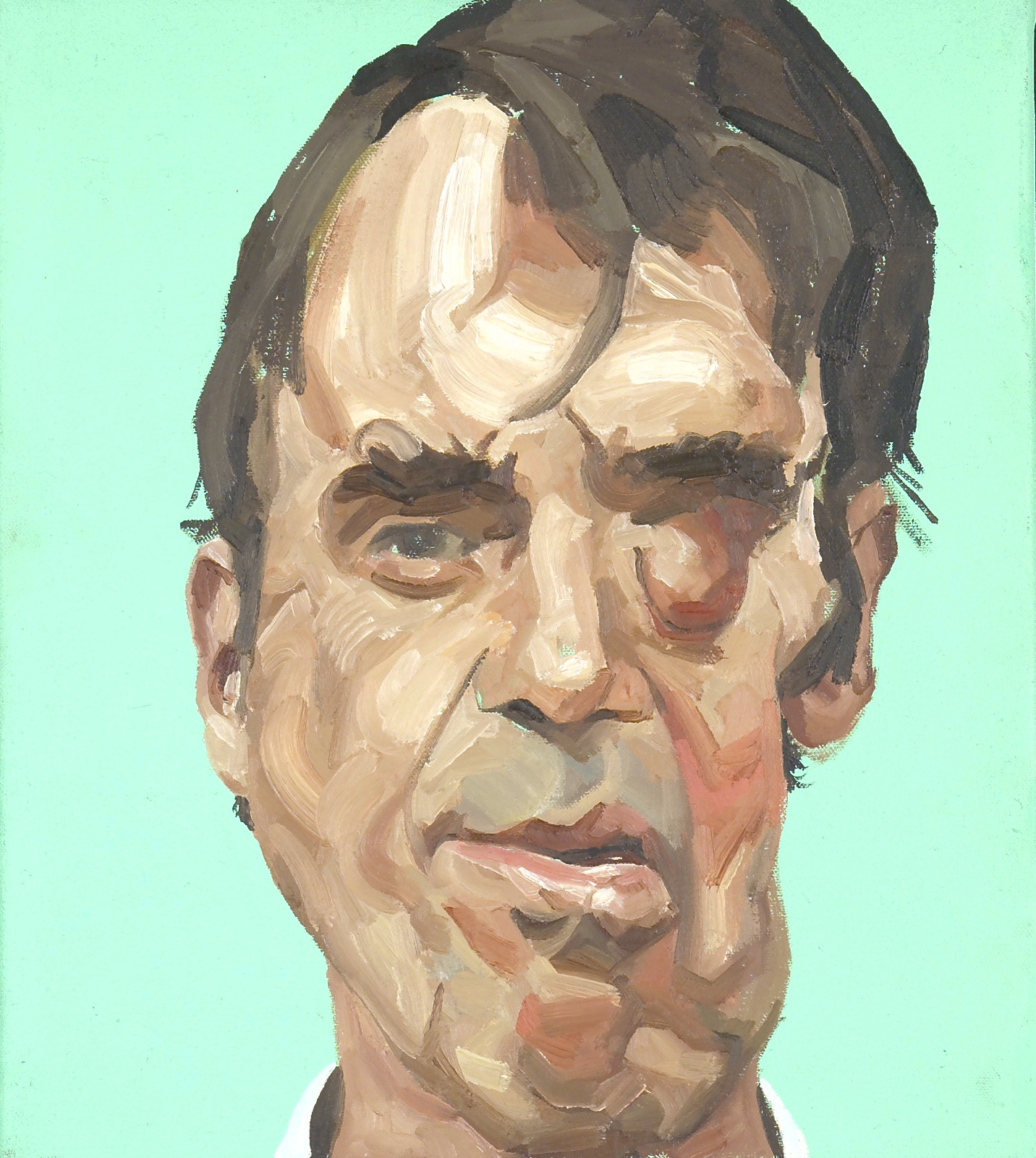
Courtesy of Mark Gilbert.
Oil on canvas, 72" by 42".
Drawing can help sharpen observation and self-awareness. When performed with one’s nondominant hand, the work does not depend on drawing skills so much as on observational skills. Students gain a reprieve from rendering a careful and detailed drawing, as they are forced to rely on observation rather than on dexterity and their preconceived notions of the subject. Comparing students’ drawings allows class members to consider different attributes that each student noticed. Different students tend to focus on different features of a portrait; these differences can be launch points from which students can practice interrogating their biases and the habits of perceptions on which they typically rely.
Sitting for a portrait can also be instructive for trainees. Sitting helps one consider the anxiety a patient might feel when being observed by a clinician, perhaps watching for clues about what the physician is thinking (see Figure 3). During clinical encounters, two or more people are together in a room, facing each other with some level of anxiety about what the other is thinking and experiencing.
Figure 3. Bill, by Mark Gilbert, 2006
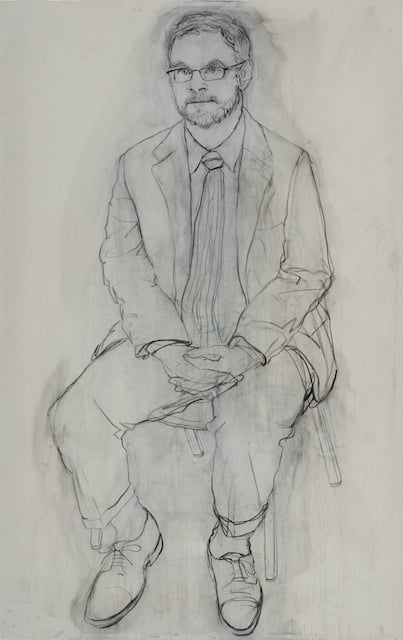
Courtesy of Mark Gilbert.
Charcoal on paper, 72" by 42".
As discussed elsewhere in this issue of the AMA Journal of Ethics, accepting and acknowledging silence present in the room can nourish connection, and this shared silence is our best hope for a patient-clinician relationship rich in therapeutic capacity. Learning to become comfortable with silence can also help trainees navigate ambiguity and uncertainty during clinical encounters and experiences in which clinicians, patients, and their loved ones try to make sense of information on which to base important health decisions. Although double-blind, randomized controlled clinical trials are the gold standard for determining the safety and efficacy of new interventions or devices, the results—even if statistically and clinically significant—cannot tell us whether to apply a given therapy to individual patients. An evidence base still requires interpretation. This dimension of the art of medicine can be practiced when one is sitting for a portrait—particularly with focused attention to one’s psychological reactions to silence, uncertainty, and ambiguity—as such reactions persist in relationships between those who care and those who are cared for.
Aita V, Lydiatt W. An introduction to the Portraits of Care. UNMC Newsroom. December 11, 2008. https://www.unmc.edu/news.cfm?match=5201. Accessed March 11, 2020.
Aita V; University of Nebraska Medical Center. Saving Faces: Art and Medicine. https://www.unmc.edu/savingfaces/. Accessed March 11, 2020.



