Case and Commentary
Nov 2012
Dr. Janus is an orthopedic surgeon who specializes in arthroscopic surgery and keeps current with medical research in his area. His goal is not only to provide the best care but also the most effective treatment at the lowest cost for his patients. Lately, he has treated many elderly patients with osteoarthritis of the knee and has noticed that this type of surgery is often a financial burden for his patients. Although the surgery is quite expensive, at $4,500 per knee, patients continue to request it, hoping to improve their mobility. In reviewing the current literature, Dr. Janus learns that the type of arthroscopic knee surgery he has been performing routinely (arthroscopic lavage and debridement) was shown in two different studies to provide no benefit over placebo; in fact, a strong placebo effect has been suggested. Dr. Janus feels that the patients he operated upon usually did improve, but he cannot rule out the placebo effect.
Mr. Marcus is a 70-year-old retiree living on his limited pension. He suffers from advanced osteoarthritis in his knees and would do anything to be able to walk more easily on his own. He says to Dr. Janus, “My best friend had this surgery last month, and he’s already getting around the golf course great. He says this surgery was the best thing he ever did for himself. I sure would love to be able to keep up with him now. What do you say, Doc, can you do this surgery for me?”
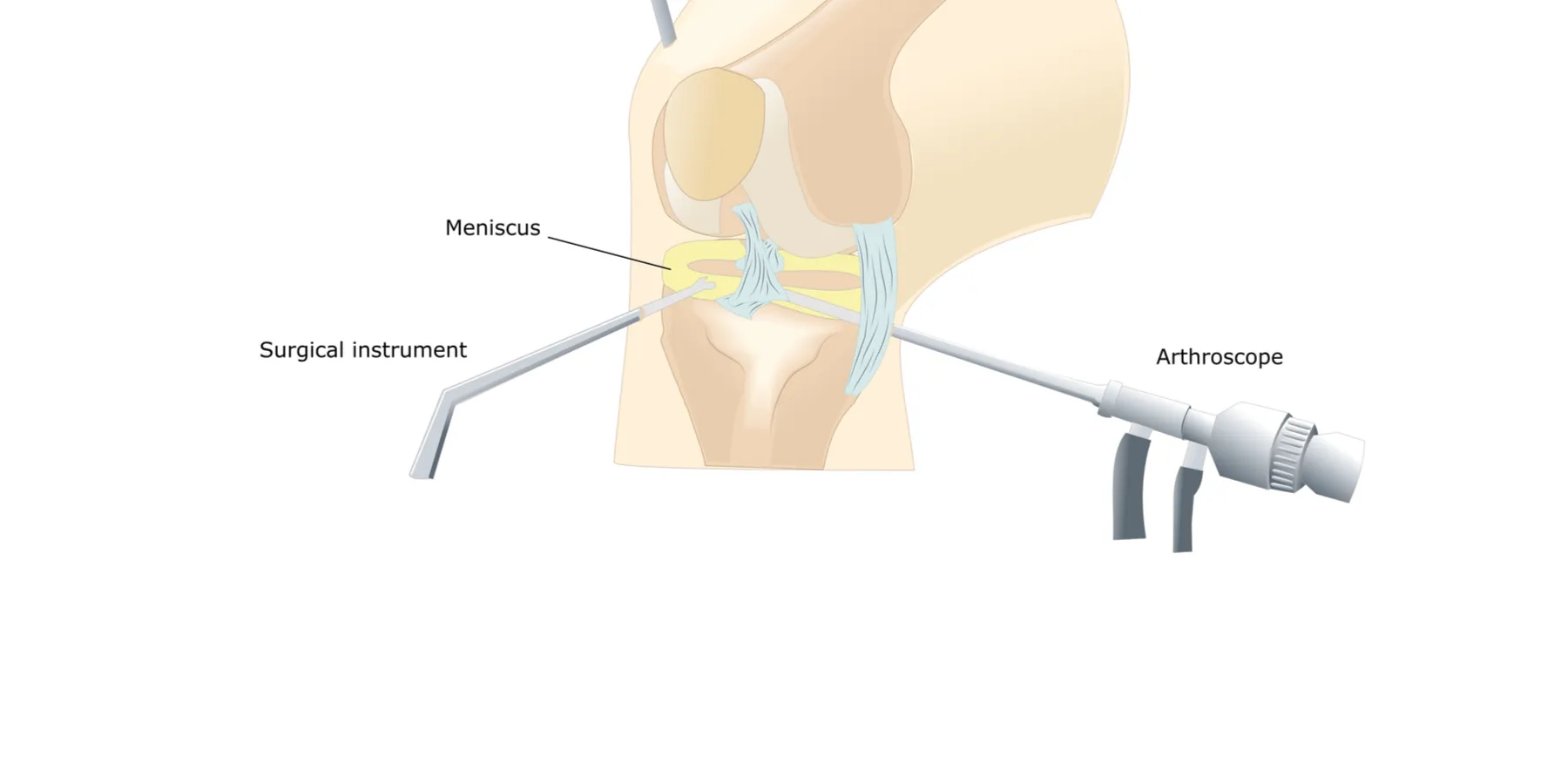
This case involves the use of a highly popular, widely employed, and generally effective surgical technique—arthroscopy of the knee. First described in 1934, arthroscopic procedures have a number of advantages over alternative approaches; they are safe, are performed in the outpatient setting, and do not preclude the later performance of more definitive surgery, such as total knee replacement [1]. As a result they are favored by patients, physicians, and medical insurers (payers) alike.
Once one of the most commonly performed of orthopedic procedures, arthroscopic debridement of the knee has come under scrutiny in recent years with the publication of two major randomized controlled clinical trials that failed to demonstrate benefit to the enrolled patients [2, 3]. Even in the current environment, with its emphasis on evidence-based medicine, such level I clinical evidence is hard to come by, particularly in the context of surgery. Nonetheless, a clinical impression endures to support the use of this procedure for osteoarthritis (OA) of the knee, albeit in a more limited, defined subset of patients.
The budget deficits and rising health care spending that have been in the forefront of the national consciousness for many years figure into the broader discussion of this case. One of the goals of the Patient Protection and Affordable Care Act of 2010 was control of the skyrocketing costs of medical care, a goal that requires the participation of physicians. Although physicians may believe that the costs of health care are largely beyond their control, the literature pertaining to regional variation in health care-related expenditures argues otherwise [4].
The issue of cost containment can be viewed in a number of ways, influenced by one’s vantage point in the system. For instance, the term “rationing” is often used by physicians who see cost-containment practices as anathema to their duty to their patients (regardless of costs); concerns relating to cost have no place at the bedside. Bioethicists have preferred the term “allocation of scarce resources,” thus framing the debate in terms of distributive justice, a foundational principal of biomedical ethics [5]. Those with an interest in health care policy see the problems in terms of systems organization, structure, and information management [6].
Regardless of how one looks at these issues, when health care resources become truly depleted, patients will inevitably be deprived of care, leaving only fairness in the distribution of the limited services to contemplate. A (partial) way out may be evolving with a recent shift in the debate from an ethics of rationing to one of waste avoidance [7]. Stimulated by Howard Brody’s “Top Five List,” [8] numerous medical societies have taken up the task of identifying those diagnostic tests and treatments that are commonly ordered but offer limited benefit. The American Board of Internal Medicine (ABIM) Foundation’s “Choosing Wisely” campaign is one example of this approach [9]. Although skepticism exists as to the long-term adequacy of this effort [10], attacking interventions of dubious benefit, estimated to account for 30 percent of the overall health care budget, appears to have caught on.
Is arthroscopic debridement of the knee one such procedure? From the standpoint of medical professionalism, we are told something of Dr. Janus’s philosophy of care—“to provide the most effective treatment at the lowest cost for his patients.” This view parallels the ethical principles emphasized by various professional societies, such as those promoted in the Ethics Manual of the American College of Physicians (ACP) [11]. This document stresses a number of professional duties among which is the physician’s obligation to society, a role acknowledging the social context in which medical care is delivered. Within this framework, decisions concerning care at the level of individual patients must consider the allocation of resources writ large, an attention that, as mentioned earlier, challenges the physician’s advocacy role. Advocacy for individual patients nonetheless has its limits, and physicians are not obligated to provide all treatments, particularly those of uncertain effectiveness.
This clinical scenario therefore provides an opportunity to marry both the application of current, evidence-based medical judgment with the need to recognize the larger imperatives currently impacting the health care system. With that said, Dr. Janus’s primary responsibility does remain his patient, in this case, to advise him about surgery.
Based on current standards of practice, he is obligated to first recommend a comprehensive program of nonsurgical management. Numerous nonoperative treatment options are available to treat patients with OA of the knee. These include activity modification, physical therapy, nonsteroidal anti-inflammatory agents, and intra-articular injections (corticosteroid or hyaluronate). All patients with symptomatic OA of the knee should be treated according to these tenets before more aggressive (surgical) methods are employed. Only for some of those who do not respond should the surgical option be considered: patients with radiographic mild arthritis or near-normal alignment but not patients with valgus configurations or arthritis in both knees [1]. So what should Dr. Janus recommend to Mr. Marcus and how should he convey it?
The case description gives limited clinical information from which to base a definitive recommendation. Nonetheless we are told that Mr. Marcus has “severe” disease in the knee(s), implying an advanced, bilateral process, clinical characteristics that are known to correlate with a poor surgical outcome. Hence, based on recent evidence, he does not appear to be a good candidate for arthroscopic surgery. Presenting this opinion to such a hopeful patient will challenge Dr. Janus’s skills of care and communication.
Since the 1970s, the literature of medical ethics has been suffused by four major principles: respect for autonomy, nonmaleficence, beneficence, and justice, the first three of which have particular relevance to this case [12]. Respect for patient autonomy means that patients have a right to request the treatment of their choice, which in Mr. Marcus’s case is to have surgery. Yet the work of caring for patients must simultaneously maximize benefit and minimize harm, goals that originate with the sometimes conflicting principles of beneficence and nonmaleficence. Dr. Janus must therefore ask himself, “Can the arthroscopy help this patient?”—a calculus that requires him to evaluate the potential benefits of the procedure in relation to the risks, while taking into account the wishes of the patient.
Although the risks of this surgery are typically small, available evidence suggests that the benefit of such surgery is likely to be low; indeed clinical experience suggests such intervention may in some instances exacerbate the symptoms and accelerate joint deterioration. Therefore, though for some patients (such as Mr. Marcus’s friend) the procedure may prove beneficial, for Mr. Marcus himself this is unlikely to be the case. Given the low likelihood of success, indeed the potential for making his condition worse, Dr. Janus should advise against surgery and advocate for a more conservative therapeutic strategy. It is critical for Dr. Janus to explain the reasoning and justification for his advice and to ensure that Mr. Marcus comprehends the explanation and, ultimately, finds it satisfactory.
Dodson C, Marx RG. Is there a role for arthroscopy in the treatment of knee osteoarthritis? In: Wright JG, ed. Evidence-Based Orthopaedics: The Best Answers to Clinical Questions. Philadelphia, PA: Elsevier; 2008:630-633.
Beauchamp TL, Childress JF. Principles of Biomedical Ethics. 6th ed. New York: Oxford University Press; 2008.
American Board of Internal Medicine Foundation. Choosing Wisely. http://www.abimfoundation.org/Initiatives/Choosing-Wisely.aspx. Accessed October 4, 2012.
Jonsen AR, Siegler M, Winslade WJ. Clinical Ethics: A Practical Approach to Ethical Decisions in Clinical Medicine. 6th ed. McGraw-Hill, 2006.