Art of Medicine
May 2020
Some patients’ stories can be hard to tell and hard to listen to, especially in pressured, time-pinched clinical environments. This difficulty, however, doesn’t absolve clinicians from a duty to try to understand patients’ stories, interpret their meanings, and respond with care. Such efforts require clinical creativity, full engagement, and the recognition that emotions and personal feelings leak into the space between storyteller and story listener. Art objects are complex bodies of information that can challenge clinicians and trainees to become more comfortable with messy narratives as well as with ethical and aesthetic ambiguity. By slowing down and observing art, trainees can reflect on how clinicians make sense of stories that contain information that appears random and lacks coherence—and, more importantly, how clinicians draw on these stories to respond to patients’ needs.
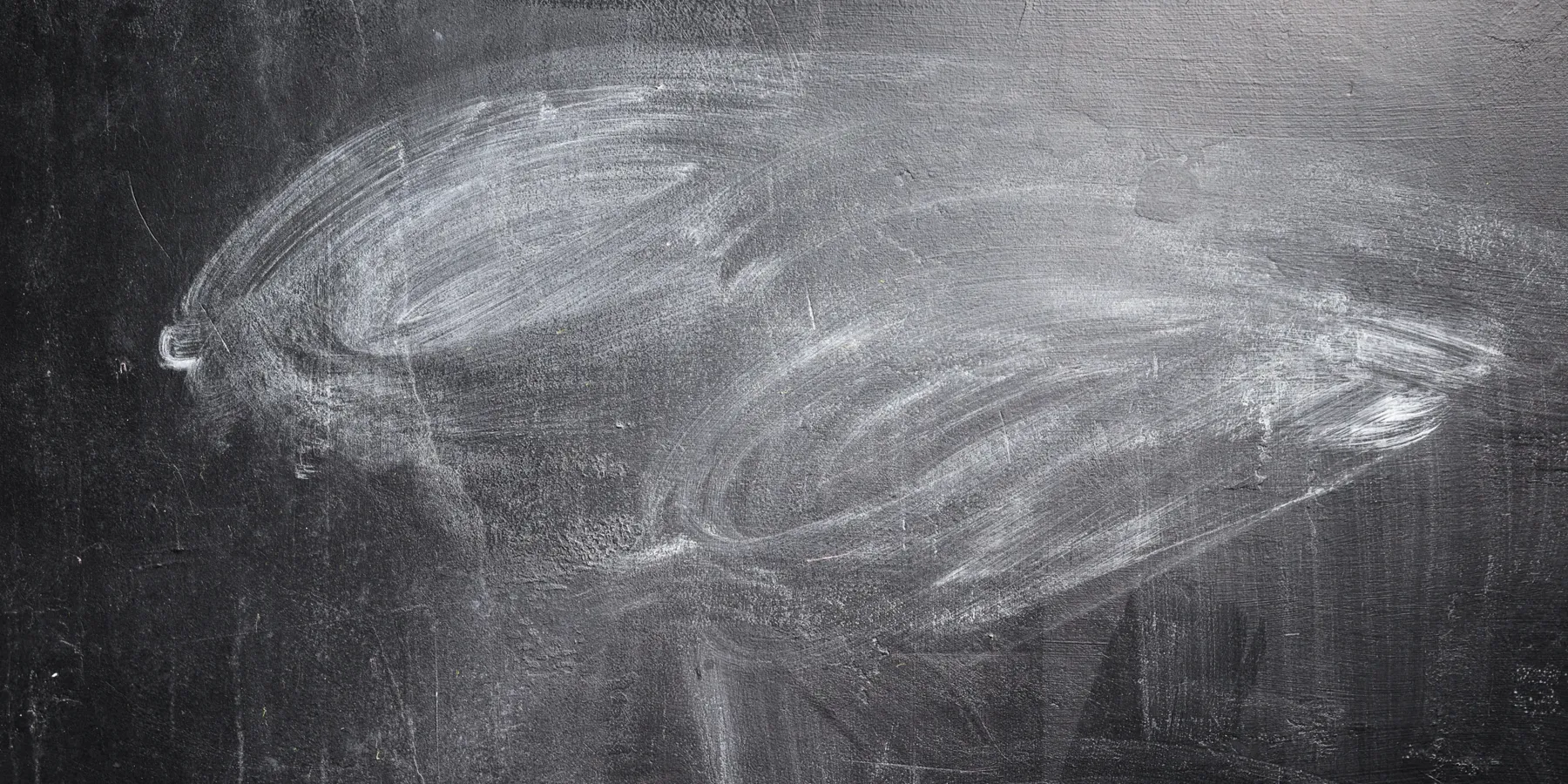
Figure. Untitled, 1968, by Cy Twombly

© Cy Twombly Foundation.
Oil and crayon on canvas.
Almost every patient encounter begins with a story. Some can be hard to tell and hard to listen to, especially in pressured, time-pinched clinical environments. That something is difficult, however, doesn’t absolve clinicians from their duty to try to understand patients’ stories, interpret their meanings, and respond with care. Clinicians’ ability to respond in ways that are true to a patient’s story and that are clinically astute and empathic necessitates assigning proper weight to what is said, how it was said, and what might have been left out, concealed, or disguised. Critical creativity—the ability to tolerate stories’ ambiguities and uncertainties—is vital when exploring the space between storytellers and story listeners, especially in clinical settings. Clinicians’ emotions and feelings can sneak into these spaces where meaning is created, influencing how fragments of information are assembled into recognizable and understandable narratives.
The American painter Cy Twombly’s Untitled, which is part of the collection at the Rhode Island School of Design (RISD) Museum, offers students, trainees, and clinicians the opportunity to become comfortable with discomfort. By slowing down their thinking, they can reflect in more granular detail upon the process whereby clinicians try to make sense of stories from what appears to be random and nonlinear information.
Students, trainees, and clinicians of various types have sat before this work of art as part of a series of collaborations between medical educators at Brown Emergency Medicine, the Warren Alpert Medical School of Brown University, and RISD Museum educators. Medical school-museum partnerships have become more common in health care education and serve many different aims, including fostering empathy and improving observation skills.1,2,3 The partnership between faculty at Brown University (with which the first and second authors are affiliated) and the museum at the RISD (with which the third and fourth authors are affiliated), which dates back to 2011, has focused on using museum objects as complex bodies of information to provoke students to think about how they think.4,5 For this discussion, we’ll focus on how this art object pushes clinicians to interrogate their reactions and responsibilities to challenging patient stories.
It’s hard to fully understand one another. People have public faces and secret, inaccessible lives. Knowing people in all their complexity and contradictions is serious and often difficult work.
Telling stories involves choices. Deciding what information to include and leave out can be a daunting task, especially for patients whose medical experiences are complicated and difficult to put into words or layered with a hornet’s nest of socioeconomic factors and mental health issues. Where patients begin their narrative can be a difficult choice that listeners accept without questioning.
Communication requires attention to what’s said and sensitivity to what’s not said.
At the RISD Museum, clinicians, students, and trainees sit before Untitled for a few minutes of quiet looking. They’re then asked what they see, what stands out for them. The Twombly painting doesn’t offer any soft landing spots for the eyes of viewers when they encounter it for the first time. One person’s starting point might be very different from someone else’s. Typically, students search for something recognizable to latch onto, a decision that involves quick and premature judgments. Are these butterflies flying off the center of the canvas? Maybe they’re hearts? Ambiguity and uncertainty breed discomfort. Reaching for labels and names is an unconscious reflex to quiet the unease. But students soon realize this and begin to understand that the inquiry demands that they operate out of that unease.
Cia Panicker (née Mathew), a former medical student at the Warren Alpert Medical School of Brown University, wrote that she “stared deeper into the chalkboard scrawls” and “found myself getting lost and frustrated at the same time. There was so much not said with this piece. There was so much left unclear. It was a mess. Twombly lives in the tension between knowing and not knowing, between communication and lack of communication. His blackboard scribbles irritated me, and now I believe that is exactly what he intended to do. He forced me [to] sit in the unknown.”6
After allowing a few minutes of quiet looking, we ask students to select a small area of this Twombly painting. They’re instructed to find a particular line or mark and make a sketch on paper, following the artist’s hand as they sketch. In this way, they get to play with the idea of positive space and negative space. Positive space is an area that has marks or information. We ask them how it feels to draw the lines, and we ask them to make a list of words to describe the experience of drawing them. They discover that creating childish-appearing and carefree lines is much harder than it appears. They also become aware of details that had previously escaped their notice. Ultimately, this exercise offers an alternative way of knowing that expands and deepens their curiosity regarding what the painting might be communicating.
Students are then asked to select an area they perceive as negative space—space around the marks, supposedly without information. Negative space, they quickly realize, is relational, in reference to something. By trying to represent the texture and the quality of the negative space, they’re forced to look more closely. They quickly notice shading or hashmarks or squiggly lines—rich visual information in spaces that they first thought were devoid of content. The group then reflects upon this experience, and we connect what they’ve learned to the task of working with words and language. We in effect ask, “When you’re listening to stories, are you sensitive to the gaps, mindful of what was unsaid—perhaps even unsayable?”
We ask students to think about a difficult conversation and to sketch a line or a series of lines that represent something important that they said or that was said to them. Consider this the positive space. What was said and why? How did the other person respond? Now depict that interaction on the page. The lines don’t need to be artistic or even straight.
The negative spaces in this interaction are addressed next. How are those represented on the page? What was communicated when they thought nothing was happening? By representing narrative experience in this manner, they begin to see how marks and their absence can communicate ideas. They become sensitive to the textures of human interaction: the tone of voice, the weight of silence, the emotional tenor, the struggle for words, the language of the body. And where were these elements vital to communication located? They were frequently drawn in the area identified as a negative space.
Many students are self-conscious about their drawing ability. We insist that artistic quality isn’t important. The focus of this exercise is to capture their thinking process on the page and to examine closely how stories are constructed and understood in medicine and in their lives. They soon discover that where we set our eyes and what we value as relevant information are decisions we make even before we think we’re making decisions.7
Through sessions such as this one, physicians in training have the opportunity to play with nonlinear and even illogical information. They become aware of what information they hold onto and why. And they notice the impact of their personal feelings on the selection process. They also learn how to communicate from inside a complicated experience.
The writer and art critic John Berger said, “I know of no other visual Western artist who has created an oeuvre that visualizes with living colours the silent space that exists between and around words. Cy Twombly is the painterly master of verbal silence!”8
Consider this short hypothetical dialogue between a physician and patient: “We’ll be discharging you from the hospital, soon,” says the doctor. “You’re going home.” “Oh, that’s ... wonderful,” the elderly patient says. She pauses. “My husband died last month.” “I’m so sorry to hear that,” the physician says, holding her hand. “Your tests were all negative. You must be excited to sleep in your own bed.”
Patients might cue their real concerns indirectly. In this case, the woman’s grief is compounded by the thought of sleeping alone in her bed and not having someone at home to care for her. One study showed that physicians often respond by neglecting these cues or by not following up and exploring these concerns further.9 They were more likely to respond to the problem underlying the emotion when the problem involved logistical or biomedical issues as opposed to grief.9 But these cues are often quiet cries for help. Surprisingly, in one study, visits with missed opportunities to address patients’ clues—direct or indirect comments about their psychological or social concerns—were longer than those when those clues were picked up.10 In another study, physicians were courteous to patients even while ignoring their more pressing existential concerns. The authors labeled this phenomenon “a moral offense.”11
Stories are rich with silences and gaps. Communication requires attention to what’s said and sensitivity to what’s not said. Perceived negative spaces are often harbors of vital and tender details. The portrait of a life in crisis might look not like a portrait but like wild and disconnected brushstrokes.
The quiet, curated museum can destabilize clinicians in training and serve as safe spaces for them to work within the uncertainty and instability of clinical practice. The moral duty to care for patients with dignity and compassion begins with caring for their story. There’s a difference between thinking about stories and thinking with stories.12 Clinicians have an ethical responsibility to sit with these stories, especially if to do so feels like grasping at the ungraspable. When patients entrust clinicians with their stories, they’re opening a window onto their struggles and complicated lives. By devaluing or ignoring what’s chaotic and confusing in a patient’s story, we devalue the vulnerable teller of the story. Not all patients expect an answer, but they all deserve a meaningful response. This can only happen when physicians possess the skills, the courage, and the creativity to explore negative space with just as much consideration and rigor as they do marks.
Blythe SG. Object lessons. In: Somerson R, Hermano ML, eds. The Art of Critical Making. Hoboken, NJ: John Wiley & Sons; 2013:116-137.
Kase S, Mathew C. From galleries to wards: a reflection. RISD Museum. https://risdmuseum.org/manual/82_from_galleries_to_wards_a_reflection. Published September 18, 2013. Accessed August 26, 2019.
Berger J; Overton T, ed. Portraits: John Berger on Artists. London, UK: Verso; 2015.
Frank AW. Letting Stories Breathe: A Socio-Narratology. Chicago, IL: University of Chicago Press; 2010.



