Case and Commentary
Dec 2024
Peer-Reviewed

This commentary on a case considers how and by whom decisions about health care structures and spaces should be made and suggests merits and drawbacks of shared decision-making as one approach to Certificate of Need assessments.
Dr A is an internist widely known for their work in evidence-based health care design. As part of a conference in design innovations in community-based health care, Dr A has been asked to lead a half-day working session for health professions students, clinicians, patient advocates, and community leaders. Dr A explains that Certificate of Need programs are means by which many states are supposed to regulate supply of health care services in their jurisdictions. Dr A then poses to audience members, “Let’s say you’re submitting a Certificate of Need application to build a new hospital. In your proposal, which features in your design drawings and descriptions will you talk about and why?”
Some audience members’ priorities focus on ventilation and waste removal streams, numbers of computer stations, and supply rooms’ proximity to patient care areas. Others suggest why features such as window sizes in patients’ rooms, access to and visibility of a garden courtyard, parking availability, sign clarity and navigability to patient care areas, locations of bathrooms and other common spaces, and easy outside access to municipal transit stops should be design priorities.
As Dr A expected, session participants identified numerous design features. The rest of the half-day, Dr A guided a discussion about how design priorities express stakeholders’ health care infrastructure needs.
One purpose of a Certificate of Need is to demonstrate public need for a proposed project. As such, a Certificate of Need purports to speak for a community and necessarily involves value propositions, a priority ranking, and decisions about community interests that a proposed project could serve. How a decision should be made cannot be divorced from who should be part of making it. We and our colleagues have argued elsewhere that health care design involves significant ethical questions and should be evidence based.1,2 Among ethical concerns at the patient level are disclosure, informed consent, and freedom of choice. Macro-level concerns include just distribution of shared, limited resources and procedural justice with respect to public goods such as representation and democratic deliberation. Expanding the group of stakeholders is about not only getting more opinions but ensuring the people affected by the decisions interact with those who have project-specific expertise. Thus, appropriately answering questions about the need for design elements begins with determining 2 things. First, who needs to be present to provide a technically informed, evidence-based answer? Second, who should have a voice in the working session in virtue of being most affected by the outcome? Hospitals are expensive and difficult to modify; any elements that would pose risks of harm or incur unjust distribution of resources will exist for decades and therefore should be carefully considered.1
Dr A has included health professions students, clinicians, patient advocates, and community leaders in the working group, but there are 4 conspicuous absences. First, while Dr A is widely known for their work in evidence-based design (EBD), that work is almost certainly avocational as far as actual design goes; Dr A is not an architect, let alone a certified health care architect with subject matter expertise in designing, planning, and constructing health care buildings.3 That means that no one in the working group has the depth of knowledge to review the plans for the new hospital, assess potential failings, and evaluate the pros and cons of competing solutions.4
Second, while there are patient advocates in attendance, there are no patients or their families in the working group. Patient advocates are not a substitute for diverse patient experience, which is recognized as an important dimension of health care, alongside clinical effectiveness and patient safety.5 Patients are heterogenous; some use the emergency department frequently but are never admitted, whereas others with chronic conditions frequently have long admissions. An admission to an intensive care unit (ICU) is entirely different from a psychiatric admission. Still others have disabilities that make movement or communication difficult. As many patients rely on surrogate decision-makers who are typically family members, family members’ hospital experiences matter. Families have experience with waiting areas and navigating public parts of the hospital—things patients themselves rarely experience. Yet family areas are often afterthoughts in facility design,6 although family members, safety,7 and good health care outcomes8 are also critical to patient well-being9 and, therefore, should be considered key parts of health care service design.10
Given the heterogeneity of patient and family experiences and the importance of family member presence in patients’ outcomes, it’s likely advantageous to involve representatives from different patient populations in working groups for specific purposes. An obstetrics wing or birth center might benefit from input from families who recently had deliveries. Former ICU patients and their families likely have insight on improving ICUs, waiting rooms, and family meeting rooms. Cardiac, pulmonary, and neurology patients and families could provide input on rehab facilities. Likewise for oncology, adolescent medicine, and pediatrics.
Third, nonclinical staff are not typically represented in design decisions. Several accounts in the literature describe a lack of space parity: hospitals have well-designed and appointed spaces for patients and families but not for staff. In particular, a documented decline in staff social spaces signals a devaluing of health care professionals and denigration of their daily work experience and productivity.11,12 Notably, there are no hospital administrators in the working group. Yet there are operational, logistic, and financial realities that must be considered for the working group to focus on realizable features rather than unachievable flights of fantasy. Hospital administrators are essential for providing knowledge of a health care system’s or campus’s overall vision and future growth strategy.
A documented decline in staff social spaces signals a devaluing of health care professionals and denigration of their daily work experience and productivity.
The first and last oversights can be remedied with the inclusion of health care architects and hospital administrators, but the second will be more difficult; a representative set of concerns would likely require analysis of surveys of patients, family members, and staff. We and our colleagues have argued that, as hospitals already have teams of people who study outcomes and report them as required to oversight agencies, it would be relatively simple to expand quality improvement metrics to include elements of the built environment.1 Even after a hospital is constructed, opportunities exist for ongoing performance assessment that can inform operational changes. For example, locked space for medication storage that serves an ICU may turn out to be insufficient to bridge resupplies from the central pharmacy, necessitating an expansion of storage near the ICU. Ongoing performance assessment can identify such shortcomings so leadership can guide investment prioritization.
At this point, we have a set of stakeholders who have the necessary expertise in EBD and those who will be most affected by the decisions. The question, Who should decide whether and how stakeholders’ needs are met? can be answered in the same way we make other decisions in health care that involve technical expertise and normative concerns: shared decision-making.
In shared decision-making, clinicians are responsible for determining the range of appropriate options based on the best available evidence or clinical judgment born of long practice and relying on the patient or duly appointed surrogate to choose from among that range of appropriate options based on their values and preferences.13 Shared decision-making frameworks have been developed for mediating authority depending on specific features of a given situation and decision. Both Opel’s 4-step framework14 and Teti and Silber’s framework13 apply this distinction.
Construction of a hospital involves many decisions that are akin to plan-of-care decisions and have myriad effects on patients, families, and staff.1 Rather than being based on the interests of a single representative patient, however, a hospital’s design and construction should result in a facility that serves the community in which that hospital is situated. The hospital might serve only a local community, or it might be part of a regional network that ensures that advanced therapies are available in all regions of a country.
Any decision-making process can be broken down into individual decision points like a plan of care. Some elements are dictated by code, for example, and are not optional; like standard care, all hospitals must meet the various requirements for safety and function. Other decisions involve normative considerations. While some hospital administrators might be tempted to install expensive artwork or sculpture to impress donors, the clinical and nonclinical staff might point out that money would be better spent on providing spaces for staff to meet and interact away from the bedside. The health care architect might point out that design can be used to improve a sense of well-being—a compelling funding priority after a New England Journal of Medicine Catalyst report noted that 83% of clinicians, leaders, and executives viewed physician job satisfaction and burnout as an ongoing issue in their organizations.15,16 If they knew of staff needs, patient and family stakeholders might agree that increasing opportunities for health care staff to interact could improve communication and therefore care coordination.17 It seems likely that Dr A’s group would not choose to spend money on or allocate space to art installations if that money could be used for design elements that improved performance of health care teams. By adapting a shared decision-making framework, decision-making authority can be organized around both value considerations and the differing epistemic standing of the stakeholders (see Figure).
Figure. Architects’ Roles in Developing the Final Design Concept
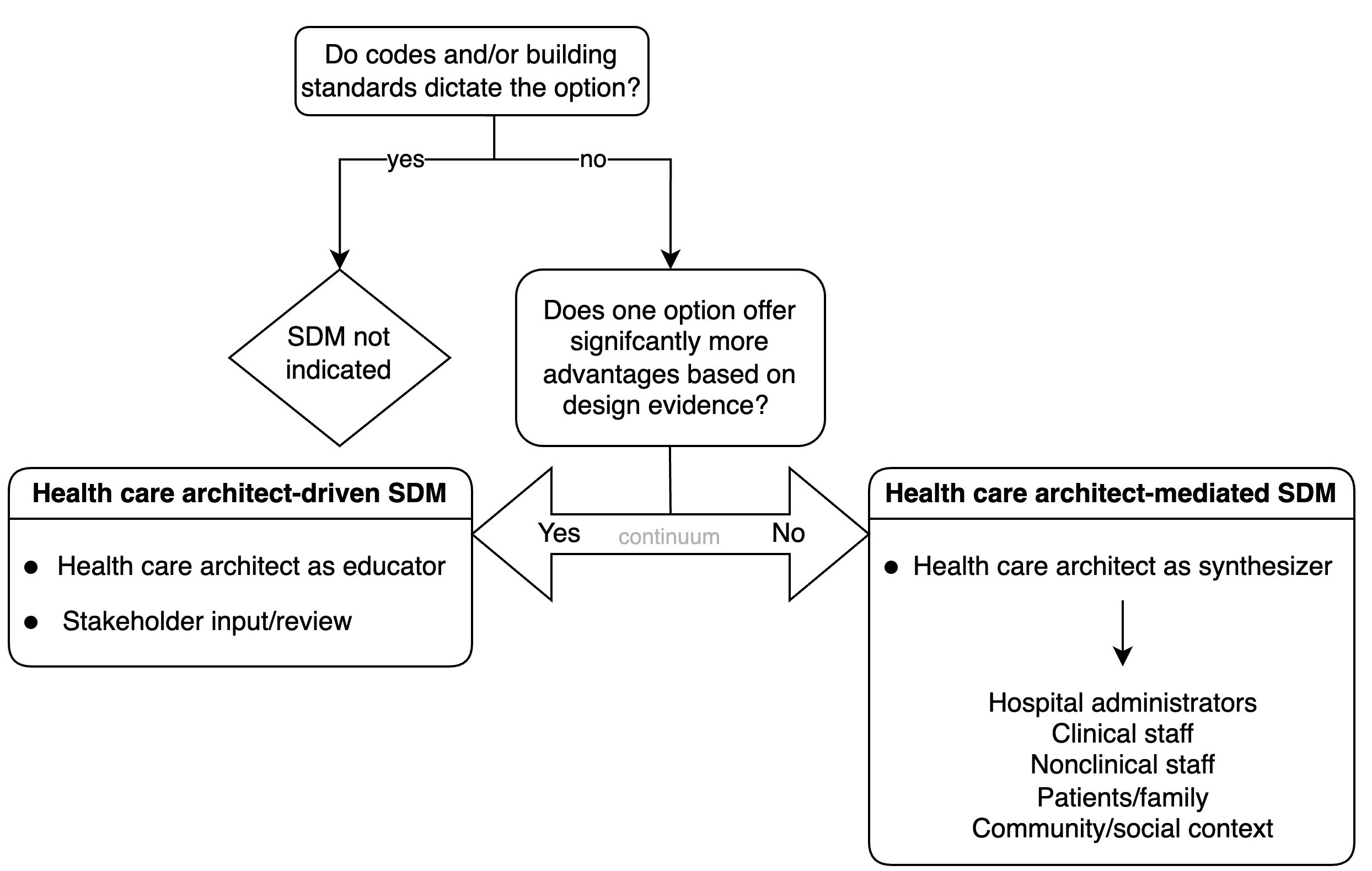
Abbreviation: SDM, shared decision-making.
Successful decision-making involves selecting from among competing choices with any evidential basis. If more than one option remains and no strong evidentiary basis exists for selecting one option versus another, employing a consensus approach with stakeholders affected by the decision is ethically appropriate (see Figure).14
Scores of decisions pose fertile ground for improving hospital operation and patient outcomes through built space in health care. Consider the following example. It is common today for disagreements to occur about myriad aspects of maternal care in hospitals: mothers’ refusal to wear fetal monitoring for fear of higher risk of cesarean section (C-section) is common in our experience, with monitoring contributing to unnecessary C-sections.18 These disagreements can lead to conflicts that result in disruption of services, poor patient experiences, and an unpleasant work environment. In the case, the health care architect on the project could direct the group of stakeholders to Ariadne Labs’ research on the causes of unnecessary C-sections.19,20 Ariadne Labs found support for the hypothesis that rates of C-sections could be partly explained by the physical layout and space design of birth facilities. The study authors posited that unnecessary C-sections could be reduced with design interventions that lessen throughput pressure in birth facilities—for example, by allocating relatively greater space to natural birth areas than operating areas. Through this evidence-based approach, the facility design could incorporate Ariadne Labs’ pressure tank model to identify design elements that influence cesarean delivery and put in place steps to mitigate pressure to move patients to C-sections apart from medical need.
To take another example: disruptions to sleep-wake cycles in older patients are known to pose health risks.21 Clustering multiple interventions that would normally be spaced throughout the night into a single encounter is a common technique to minimize room entries and exits. However, these patients and their families could work with clinicians to further improve clustered care. They might propose that task lighting be made available for nurses and techs to perform their work in darkened rooms. For charting at the bedside, computer monitors could allow for rotation away from the patient’s bed to minimize waking patients unless necessary. Some room designs allow clinicians to look into the room without opening the door. Such simple steps can confer lasting benefits.
In addition to patient care, another clear benefit of an evidence-based approach is improved operations. For example, there are opportunities to use the built environment to reduce conflict and workplace violence by applying existing research on the role of foot traffic flow, “energetic” décor, color schemes, lighting, and discomforting noise, heat, or furnishings in these behaviors.22 The color Baker-Miller Pink, for example, has been studied in relation to suppression of human aggression.23 There is already existing precedent for diminishing violence through design in numerous venues, including prisons,24 urban settings,25 and even psychiatric units wherein better design resulted in reduced aggressive behavior and improved staff safety.26
Throughout the shared decision-making process, the stakeholders could evaluate their decisions based on the hospital’s or health system’s mission, vision, and values. These often include commitments such as putting the patient first, working as a unified team, remaining dedicated to transparency and integrity, and so on. Through shared-decision-making, the built health care environment could come to exemplify these values rather than just hold billboards restating them.
A Certificate of Need must include all the elements required by code and jurisdiction, but the purpose of the requirement is to ensure that all proposed building projects meet a need of the community. The goal is to protect existing communities from unfettered development that might contribute nothing to or might damage the fabric of the community. Accordingly, the proposal should address the specific site of the project and any challenges or benefits it has. The proposal should also account for the infrastructure demands of a new hospital: are sufficient power, water, and other resources available? How will developing the site affect existing traffic, and will there be sufficient parking? One challenge is that paying for parking can become very expensive for families who come daily to visit patients with long hospital stays, and this expense can disadvantage patients whose families have limited resources. Benefits to be considered are whether the proposal includes specialty services aligned with the needs of the community (eg, older or younger, urban or rural). An ethically informed proposal that takes into account the views of proposed stakeholder groups would explain how the hospital design is inclusive of different cultures and faiths and if there is a specific community the hospital is intended to serve. For example, if the hospital serves a community in which large families are common, family meeting rooms should accommodate those larger families and make them feel welcome. If the setting is rural or offers advanced services patients travel for, such as organ transplant, affordable accommodations should be located nearby. Inclusion of representative stakeholders in a process of shared decision-making that mediates decisional authority can promote ethically informed, evidence-based hospital design practices, leading to improved building performance and health outcomes.
Anderson DC, Hercules B, Teti SL. The bioethics of built healthcare spaces. Hastings Bioethics Forum. January 13, 2021. Accessed May 8, 2024. https://www.thehastingscenter.org/the-bioethics-of-built-health-care-spaces/
Becoming certified. American College of Healthcare Architects. Accessed July 29, 2024. https://healtharchitects.org/becoming-certified/
Hamilton DK, Pentecost AR 3rd, McKahan D. ACHA evolves with the health care design profession. American College of Healthcare Architects plays a vital role in maintaining the profession’s integrity. Health Facilities Management Mag. Feb 1, 2017. Accessed May 8, 2024. https://www.hfmmagazine.com/articles/2676-acha-certification-stands-test-of-time
DiNardo A. Family and visitor spaces: an opportunity to innovate. Healthcare Design Mag. June 6, 2014. Accessed May 8, 2024. https://healthcaredesignmagazine.com/trends/architecture/family-and-visitor-spaces-opportunity-innovate/
Prior SJ, Campbell S. Patient and family involvement: a discussion of co-led redesign of healthcare services. J Particip Med. 2018;10(1):e5.
Landy J. How architects ruined healthcare. Globe and Mail. May 24, 2019. Accessed May 8, 2024. https://www.theglobeandmail.com/opinion/article-how-architects-ruined-healthcare/
Teti SL, Silber TJ. Parental permission, childhood assent, and shared decision-making. In: Nortje N, Bester JC, eds. Pediatric Ethics: Theory and Practice. Springer Nature; 2022:111-125.
DiNardo A. Workplace meets healthcare: mix & match. Healthcare Design Mag. June 17, 2019. Accessed May 8, 2024. https://healthcaredesignmagazine.com/trends/architecture/workplace-meets-healthcare-mix-match/
Swensen S, Strongwater S, Mohta NS. Leadership survey: immunization against burnout. NEJM Catalyst; 2018. Accessed May 8, 2024. https://qi.elft.nhs.uk/wp-content/uploads/2018/04/Immunization-Against-Burnout_Swenson-2018.pdf
O’Daniel M, Rosenstein AH. Professional communication and team collaboration. In: Hughes RG, ed. Patient Safety and Quality: An Evidence-Based Handbook for Nurses. Agency for Healthcare Research and Quality; 2008:chap 33.
Ledbetter A. C-section rates are way too high. We need to hold doctors and hospitals accountable. Scientific American. July 21, 2023. Accessed September 11, 2024. https://www.scientificamerican.com/article/c-section-rates-are-way-too-high-we-need-to-hold-doctors-and-hospitals-accountable/
Shah N. Designing capacity for high value healthcare: the impact of design on clinical care in childbirth. Ariadne Labs; 2015. Accessed May 8, 2024. https://www.ariadnelabs.org/wp-content/uploads/2017/04/170223_Ariadne-Report_Final.pdf
Shah N, Barker K. Doctor-architect collaboration explores whether hospital design impacts care during childbirth. Ariadne Labs. December 14, 2015. Accessed May 8, 2024. https://www.ariadnelabs.org/resources/articles/doctor-architect-collaboration-explores-whether-hospital-design-impacts-care-during-childbirth-2/
Conflict and violence in pubs: design issues. MCM Research; 1992.
Irish J. The surprisingly dark history of the color pink. Fast Company. September 28, 2018. Accessed September 11, 2024. https://www.fastcompany.com/90243505/the-surprisingly-dark-history-of-the-color-pink
How Norway turns criminals into good neighbours. BBC. July 6, 2019. Accessed May 8, 2024. https://www.bbc.com/news/stories-48885846
Shepley M, Sachs N, Sadatsafavi H, Fournier C, Peditto K. The impact of green space on violent crime in urban environments: an evidence synthesis. Int J Environ Res Public Health. 2019;16(24):5119.
Ulrich RS, Bogren L, Gardiner SK, Lundin S. Psychiatric ward design can reduce aggressive behavior. J Environ Psychol. 2018;57:53-66.



