Case and Commentary
Dec 2024
Peer-Reviewed
When built environments in health care result from an evidence-based design (EBD) process, they are interventions that can improve patients’ health outcomes. This commentary on a case discusses which ethical values should guide organizations’ capital expenditure decisions about retrofits, which might be more costly than the original budget. This discussion urges reevaluation of the common assumption that capital improvements are “sunk costs,” since such improvements can promote long-term positive health outcomes for an organization’s patients, thereby advancing both financial value and ethical values. This commentary also suggests that EBD offers key interventions that are clinically and ethically relevant.
A large health system has contracted with an architectural firm to develop plans for renovations of one of its hospitals. Originally built in the late 1960s, the building is in an urban-based community. During a planning meeting, the architect considers suggesting incorporating a white noise sound system, other sound-masking equipment, and good lighting in the design plans, since there is evidence that these features promote more peaceful inpatient environments. Despite the likelihood that these retrofits would improve patients’ experiences, the architect is concerned that they will cost far more than the contract’s budget allocates and wonders whether to suggest the retrofits.
When renovating a facility, stakeholders have an opportunity—and an ethical obligation1—to do more than base decisions on personal preferences and budgets. Health care organizations undertaking a facility design project should require an evidence-based design (EBD) process, wherein the team bases “decisions about the built environment on credible research to achieve the best possible outcomes.”2 The long-term benefits of improved outcomes should shift the view of the project from being a “sunk cost” (ie, a cost that will never be recovered) to being an investment with the potential for payback over the usable life of the project. The return is calculated based not only on hard “dark green” dollars (ie, measurable financial outcomes, such as resource use, length of stay, and staffing), but also on soft or “light green” dollars (ie, harder-to-quantify organizational consequences, such as reputation, patient and staff satisfaction, and workplace safety).3 Accordingly, the priority in renovating a facility shifts from How much should we spend? to What design decisions will contribute to improved clinical performance and improved financial outcomes? Furthermore, just as clinical ethical principles are applied to medical practice,4 so they can equally be applied to the practice of facility design. We should also ask: What is our obligation to align design decisions affecting care delivery with the principles of beneficence, nonmaleficence, autonomy, and justice? and How do we value such design decisions (literally and figuratively)? This article describes a framework for decision-making about EBD renovations that are both clinically relevant and ethically sound.
The first step in meeting the obligation for renovations that improve clinical outcomes is to identify challenges in the project, including environmental conditions and ethical tensions, and to define the problems that need solving. In this case (hypothetically illustrated in the Figure), there are a host of design features that influence conditions of noise and light, as well as other environmental conditions that might lead to undesirable health-related outcomes.
Figure. Fictional 1960s Medical-Surgical Unit
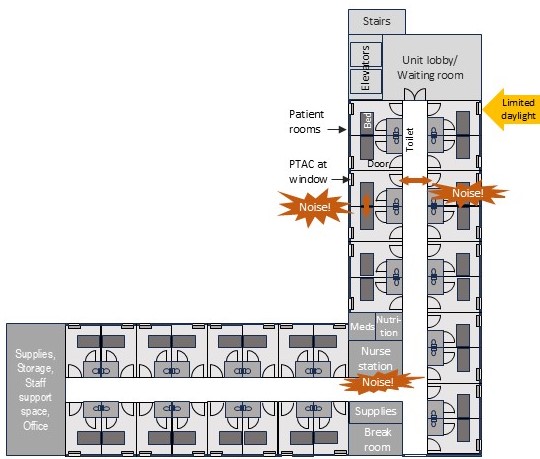
Abbreviation: PTAC, packaged terminal air conditioner.
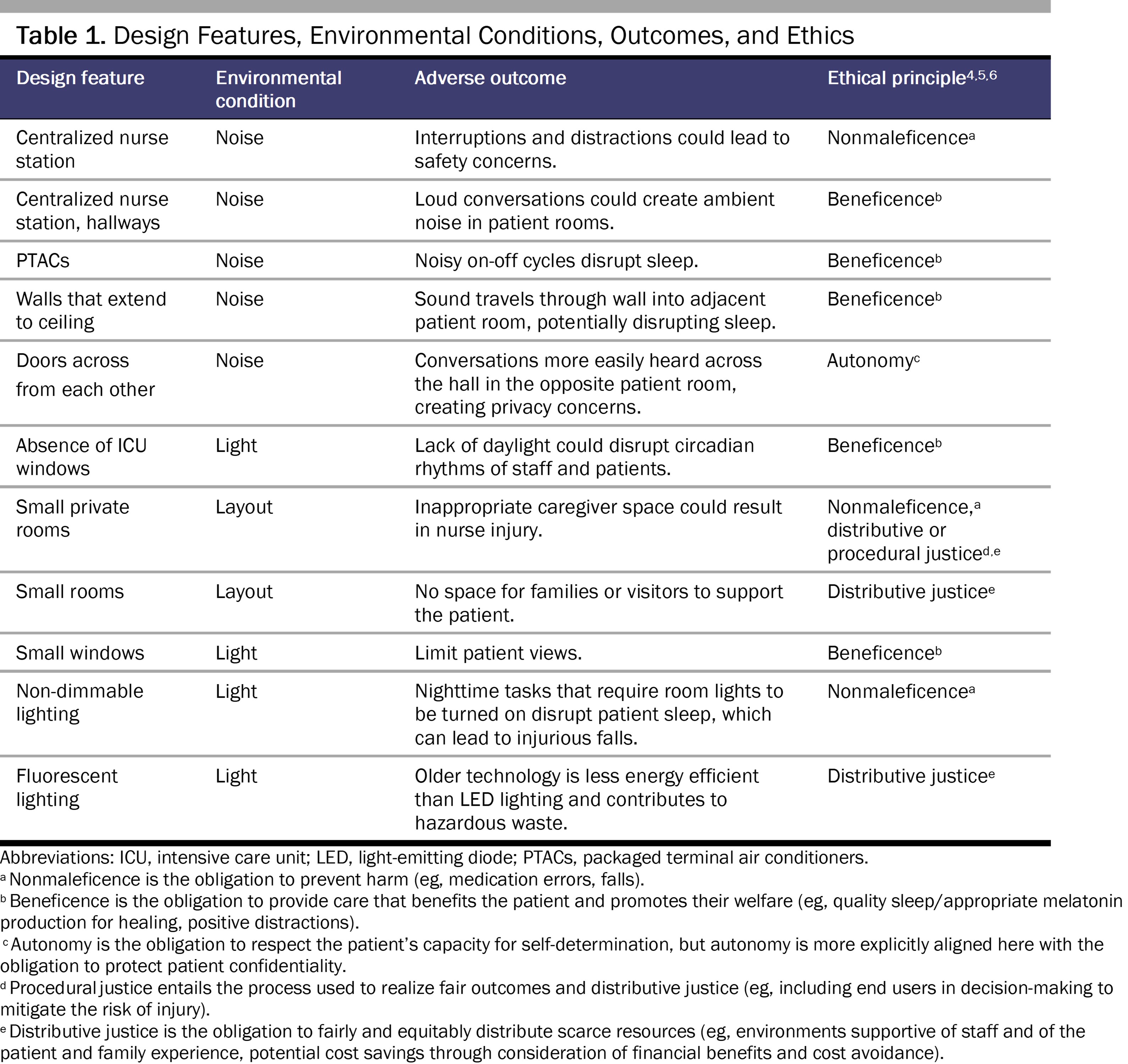
While noise and lighting are identified challenges, these are not the final outcomes of interest. The environmental conditions should be considered in the context of adverse health-related outcomes to first identify clinical ethical principles relevant to possible solutions (see Table 1).
Because built environments contain features that directly or indirectly influence health,7 an essential component of an EBD process is to examine the existing evidence of environmental conditions, such as noise and light, related to outcomes of interest in order to identify design opportunities for improving care that align with clinical ethical principles.
Noise. Noise is most consistently referenced in the context of disrupted sleep, but hospital noise is also linked to speech privacy, cognitive processing, and even posthospital syndrome.8,9,10 Noise also affects nurse anxiety, stress, and burnout.11 Noise is so important that it is included in national patient experience surveys—the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS)—that are collected and publicly reported for nearly every US hospital.12 HCAHPS scores have been shown to be influenced by minimum sound levels,13 as well as by the occurrence rate of peak sound levels.13,14 The “quiet at night” question, a proxy for quality sleep,15 has been one of the lowest performance scores since the survey’s inception. According to 2023 data, only 62% of patients reported that the area around their room was always quiet at night.16 Supporting the principle of beneficence, research has demonstrated that white noise (eg, ocean sounds) can improve sleep,17 which can reduce depression18 and heart rate19 for some patient populations.
Light. Like noise, lighting can also contribute to disrupted sleep10,20,21 and negative health outcomes resulting from disrupted circadian rhythms.22 Good lighting might be defined in a number of ways. In addition to providing appropriate light levels for tasks with energy-efficient fixtures, the nonvisual biologic effects of lighting should be considered in the early phases of hospital design. Research suggests that using dynamic lighting (eg, circadian, tunable) can improve sleep duration for some patients,21 thereby supporting the principle of beneficence. Blue-depleted lighting might result in less suppressed melatonin levels, increased sleep time, increased rapid eye movement sleep, and lower neurocognitive arousal.23 Accordingly, the Society of Anesthesia and Sleep Medicine has called for patient sleep optimization measures in patient care guidelines.24
Furthermore, modern lighting technology is more energy efficient, using perhaps 40% less energy than older florescent fixtures.25 In this case, it is fortuitous that the same dynamic lighting design intervention might support independent goals of attaining sustainability targets (eg, energy efficiency) and improving the patient experience (eg, quality sleep). This example illustrates a common occurrence in the EBD process, wherein a design intervention may influence multiple outcomes that may or may not be mutually exclusive. In the context of distributive justice, potential cost savings can be considered in future resource allocation decisions.
Light and noise can also contribute to medication errors that affect patient health and safety, adding to an economic burden associated with increased length of stay, death, and use of postdischarge resources.26 Additionally, as indicated above, light and noise can result in disrupted sleep, and sedative hypnotic drugs prescribed for sleep-wake dysfunction can have adverse effects, including falls and delirium.27
One aim of an EBD business case is to weigh costs of construction against returns for alternatives that contribute to improved outcomes. In a theoretical example of a business case for better health care design, researchers estimated cost avoidance of adverse events to offset incremental costs of construction, resulting in a simple payback period of 1 to 3 years.28,29 The EBD business case recognizes that improved outcomes and reducing avoidable harm are inseparable from the life-cycle cost of operations. This approach, which takes into account both financial and ethical value, provides an additional opportunity to consider the alignment of solutions with ethical principles.
Cost. Construction costs are often called first costs, but there are operating (life-cycle) costs (eg, maintenance, replacement) to be considered as well. Newer approaches to aid decision-making aim to forecast the long-term costs of construction and ownership (costs and revenues) over the estimated building lifespan.30 This holistic approach is better suited to a broad concept of financial value that can be realized in indirect social and ethical outcomes, as well as in direct monetary outcomes. Projects can be compared using net present value (NPV), a discounted cash flow that reflects the time-value of money, with a higher NPV reflecting a higher rate of return.31 The discounted payback allows a ranking of alternatives so that organizations can more objectively decide which projects to pursue and the opportunities that may be lost through choice selections (the opportunity cost). There is a myriad of deterministic and probabilistic methods that can be used to create financial models.7 While NPV typically applies to projects, it can also apply to individual decisions within a facility design project. As discussed below, part of the outcomes-related decision should include consideration of clinical ethics.
Value the values. Organizational values in the form of a vision statement and guiding principles, which often include the patient experience and safety, often drive projects. Nevertheless, short-term priorities, such as the project budget, easily dominate design decision-making. Containing the budget is one organizational value and aims to protect and preserve the distribution of resources across organizational imperatives, but there is rarely (if ever) a consideration of bioethical principles. In this case, the architect is reluctant to suggest design interventions with known positive effects solely due to containing the budget, one value among many. Is it ethical to ignore the potential influence of design on improved health and outcomes? Who has the responsibility to raise the issues? Do we really value the patient experience beyond marketing language? An EBD process that includes a truly interdisciplinary team (with bioethicists) could create a space for ethical discussions that frame the desired outcomes. However, advocating for ethical design interventions that are known to influence outcomes could be even more powerful when accompanied by the EBD business case. Valuing the values might aid in resolving the potential conflict between ethical and traditional business decision-making principles.
Valuing solutions. For this case, the team will need to consider the scope of improvements, their incremental costs (the amount in excess of the “standard” condition), and the benefits associated with improved outcomes. For noise, the team should evaluate the best solutions to mask the most disruptive sources commonly identified in the literature (eg, staff conversations). The cost of a noise-masking system would be evaluated against the potential for beneficence (eg, improved health and welfare), as well as higher HCAHPS scores that might lead to higher reimbursement from the Centers for Medicare and Medicaid.32,33 This financial benefit would help turn light green dollars into dark green dollars. For lighting, the team should consider that reduced energy use with modern light-emitting diode lighting results in lower utility costs, such that the new lighting could pay for itself over time. Funding might also be obtained through energy grants, incentives, or rebates. However, in the EBD business case, while reduced energy use directly affects operating costs, the indirect costs of ethical medical care (eg, improved sleep) might be valued with respect to reduced prescriptions to improve hospital sleep,34,35,36 reduced posthospital syndrome, and reduced follow-up care.10,37 While savings from improved health-related outcomes might be light green dollars, they are important considerations for ethical medical care that can also lead to dark green dollars in the avoidance of 30-day readmission reimbursement penalties.38
With EBD, the interdisciplinary team can make informed decisions related to interventions and outcomes. While no project can incorporate every idea, the framework of the business case offers the opportunity for a more evidence- and ethics-informed decision-making process. A process to pursue the EBD business case is presented in Table 2.
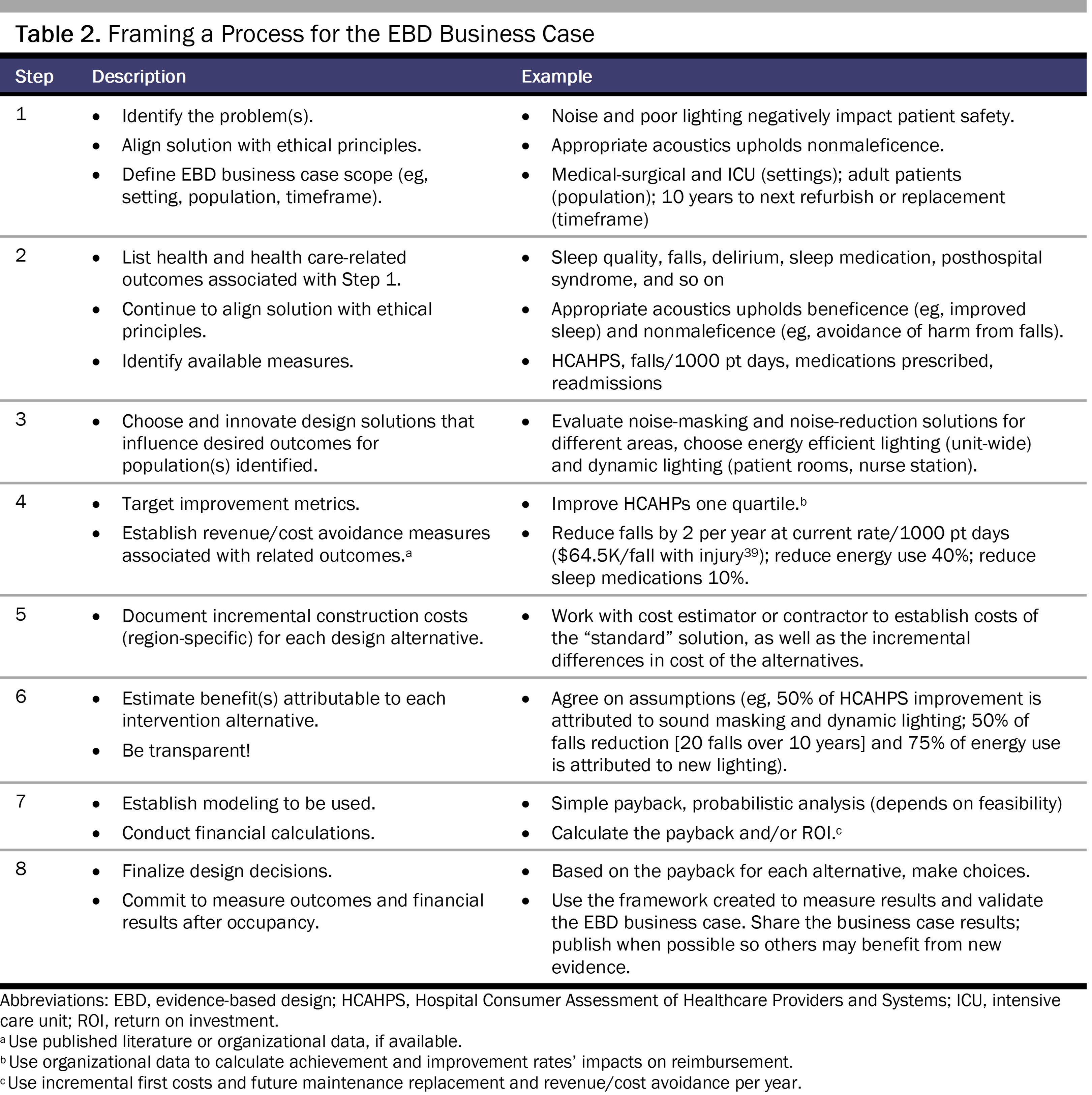
Teams should discuss calculation methods based on their feasibility and the goal of creating a narrative, a deterministic analysis, or a probabilistic assessment.39
EBD processes for health care facilities regard design as an intervention to improve outcomes. While the evidence base for design has been growing, the related EBD business cases, like the ethics discussions in design, are sparse. While health care organizations focus more often on the dark green dollars of tangible choices than on the light green dollars that result from societal value and improved health outcomes, facility project stakeholders (eg, architects, designers, clinicians, health care governing bodies) have a responsibility to consider design decisions in the context of medical ethics. Developing a business case for built environment interventions can be complicated, however. There is rarely a one-to-one relationship of interventions and outcomes; there are moderating and confounding variables; and, unfortunately, there is a lack of easily accessible data. However, in order to best provide patients and staff with safe and health-promoting environments, decision-making must balance the ethics of improving outcomes with the recognition there will be not only short-term costs but also long-term financial implications. What is built today does not end with construction; there is an ethical imperative for investments that can promote health and mitigate the risk of negative outcomes for many years to come.
About EBD. Center for Health Design. Accessed December 26, 2023. https://www.healthdesign.org/certification-outreach/edac/about-ebd
Institute for Healthcare Improvement; National Patient Safety Foundation. Optimizing a business case for safe health care: an integrated approach to safety and finance. Institute for Healthcare Improvement; 2017. Accessed May 15, 2024. https://www.ihi.org/sites/default/files/2023-10/OptimizingBusinessCaseSafeHealthCare.pdf
Beauchamp TL, Childress JF. Principles of Biomedical Ethics. 5th ed. Oxford University Press; 2001.
Dauda B, Denier Y, Dierickx K. What do the various principles of justice mean within the concept of benefit sharing? J Bioeth Inq. 2016;13(2):281-293.
HCAHPS: patients’ perspectives of care survey. Centers for Medicare and Medicaid Services. Updated September 6, 2023. Accessed July 10, 2024. https://www.cms.gov/medicare/quality/initiatives/hospital-quality-initiative/hcahps-patients-perspectives-care-survey
Gulati J, Arora V, McDaniel L, Affini M, Mason N, Orlov N. Which hospitals promote a sleep-friendly patient experience? J Patient Exp. 2023;10:23743735231151544.
Patient survey (HCAHPS)—national. Centers for Medicare and Medicaid Services. April 24, 2024. Accessed July 22, 2024. https://data.cms.gov/provider-data/dataset/99ue-w85f
Yoon H, Baek HJ. External auditory stimulation as a non-pharmacological sleep aid. Sensors (Basel). 2022;22(3):1264.
Pamuk K, Turan N. The effect of light on sleep quality and physiological parameters in patients in the intensive care unit. Appl Nurs Res. 2022;66:151607.
Vethe D, Scott J, Engstrøm M, et al. The evening light environment in hospitals can be designed to produce less disruptive effects on the circadian system and improve sleep. Sleep. 2021;44(3):zsaa194.
Boussabaine A, Kirkham R. Whole Life-Cycle Costing: Risk and Risk Responses. John Wiley & Sons; 2008.
Hoogmartens R, van Passel S, van Acker K, Dubois M. Bridging the gap between LCA, LCC and CBA as sustainability assessment tools. Environ Impact Assess Rev. 2014;48:27-33.
Richter JP, Muhlestein DB. Patient experience and hospital profitability: is there a link? Health Care Manage Rev. 2017;42(3):247-257.
Hospital Readmissions Reduction Program (HRRP). Centers for Disease Control and Prevention. Updated September 10, 2024. Accessed September 13, 2024. https://www.cms.gov/medicare/quality/value-based-programs/hospital-readmissions
Dykes PC, Curtin-Bowen M, Lipsitz S, et al. Cost of inpatient falls and cost-benefit analysis of implementation of an evidence-based fall prevention program. JAMA Health Forum. 2023;4(1):e225125.



