In the Literature
Mar 2024
Peer-Reviewed

This article canvasses extant literature about values, evidence, and standards for inpatient psychiatry units’ design. It then analyzes apparent trade-offs between quality of care and access to care using empirical and ethical lenses. From this analysis, the authors conclude that standards for the built environment of inpatient psychiatric care should align with patient-centeredness, even if a downstream consequence of implementing new patient-centered designs is a reduction in beds, although this secondary outcome is unlikely.
Inadequate access to inpatient psychiatry has received outsized attention in both the academic and the popular press compared to the quality of care provided in these settings.1,2,3,4 News reports describe prevalent boarding of patients in the emergency room, concluding directly or through implication that more psychiatric beds would lead to better population health outcomes.1,4 This assumption reflects a privileging of access to a bed over its therapeutic value—a position for which there is little empirical or ethical justification. Over a century’s worth of testimony and narrative reveals concerns about the quality and even iatrogenic harm of inpatient psychiatric care.5,6,7,8,9,10,11,12,13,14 While conditions may have improved since the 1950s, patients continue to raise concerns about dehumanizing aspects of modern inpatient psychiatric care settings, both regarding the built environment and the treatment they receive on an interpersonal level.7,14,15,16,17 Moreover, evidence suggests that minoritized and disenfranchised patients are more likely to receive care at inpatient psychiatric facilities with higher rates of complaints and episodes of restraint and seclusion,18 highlighting the social justice implications of continuing to sideline quality of inpatient psychiatric care. Given this evidence, it seems unreasonable to prioritize the expansion or preservation of psychiatric beds over the utility (ie, quality) that such care has for the patient, the central stakeholder.
In this paper, we describe the need to adopt national standards for patient-centered built environments, implementation of which will raise the floor for what we consider acceptable care and enable subsequent efforts to systematically implement patient-centered environments.
Patient-centered care—respecting patients’ needs, preferences, and autonomy—is a value19 identified by health care consensus bodies, such as the Institute of Medicine, similar to the values of safety and effectiveness.20 In the context of inpatient psychiatry, principles of patient-centered care can be seen in evidence-based, trauma-informed care models; these models are effective in preventing and reducing violence, trauma, restraint, and seclusion in inpatient psychiatric settings.21,22,23,24 Patient-centered inpatient psychiatric care has also been associated with improvements in patients’ trust in mental health professionals, their willingness to engage in postdischarge care, and the likelihood that they will have an outpatient visit within 30-days of discharge.25 Patient-centered care is, therefore, both an outcome that we value in its own right and a factor that is related to other desirable outcomes (eg, safety, engagement with care). In what follows, we will describe how patient-centered care values can be embedded within the built environment through specific design features and how the implementation of these design features can be enabled by clear standards that articulate their foundational importance.
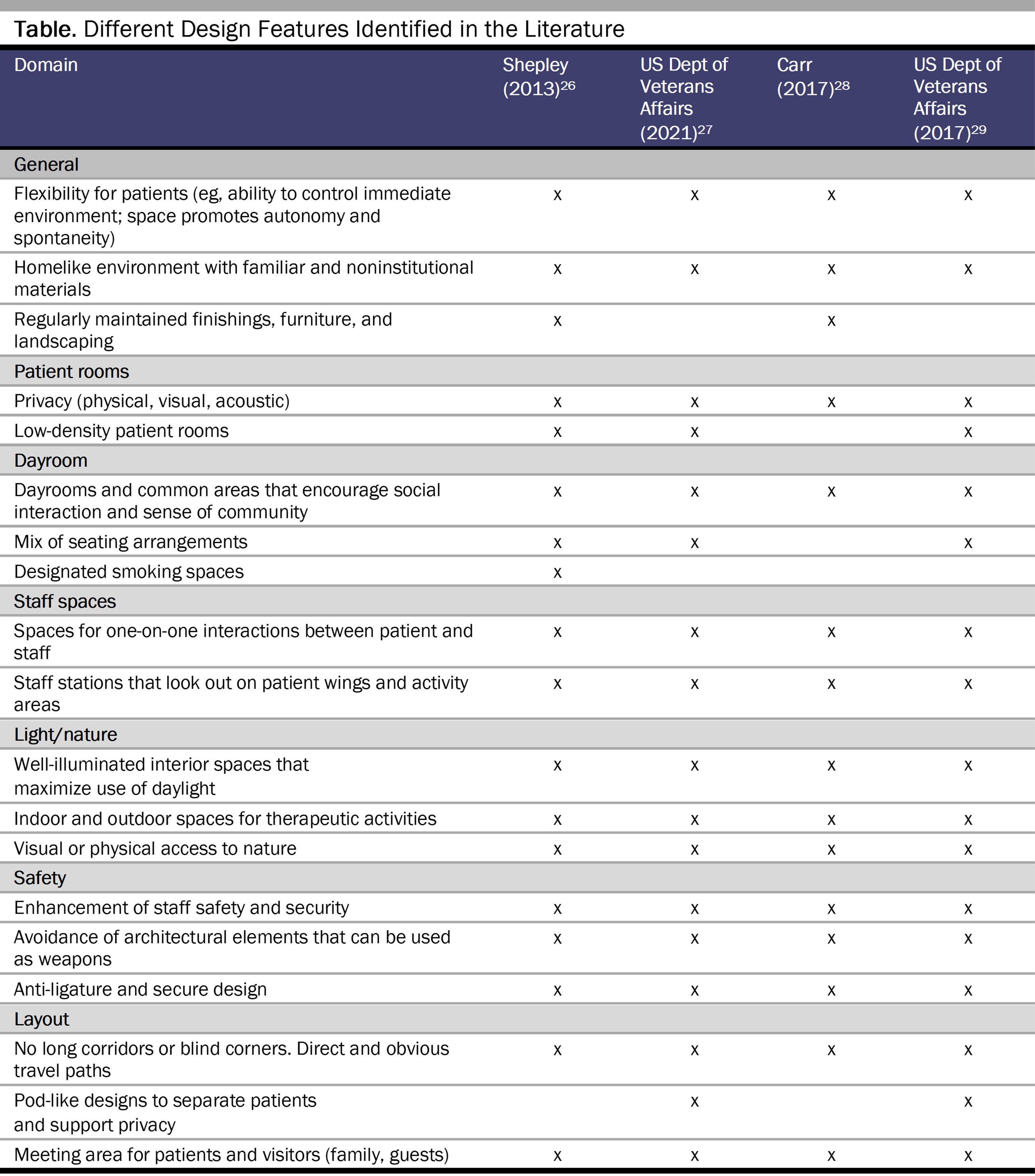
Patient-centered design features. While patient-centered care is often discussed within the context of interpersonal relationships, operationalizing patient-centered care relies on many structural components, including facilities’ built environments. We identified several features of patient-centered design relevant to inpatient psychiatry in the literature (See Table).26,27,28,29 These features range from hallways’ structures, to unit décor, to accessibility of nature. The fundamental objectives of these features are to support patients in feeling safe, comfortable, and reasonably autonomous (eg, able to control their environment and have their privacy respected). Although complete autonomy and choice in these settings may not always be appropriate, evidence suggests the importance of maximizing choice through a trauma-informed lens in order to mitigate institutionalization’s negative consequences and maximize its potential benefits.30
Standards for patient-centered design. Standards are a foundational instantiation of our values of care quality; they can be understood as the institutional or procedural counterparts of clinical recommendations or practice guidelines. They are intended to reflect our values as a society and the latest evidence, articulating a baseline floor for quality and informing subsequent accountability parameters. We evaluated language in standards outlined by leading national clinical professional and other organizations (the American Medical Association,31 the American Psychiatric Association,32 the American Psychological Association,33 and the National Fire Protection Association34,35) and regulatory bodies (the Joint Commission,36 the Centers for Medicare and Medicaid Services,37 and the Patient Safety Authority38), with respect to principles of patient-centered care as they apply to the built environment. We found little clinical professional association language related to the built environment that could further patient-centered care. The language of the National Fire Protection Association and regulatory bodies like the Joint Commission focuses primarily on fire safety and access to ligature points.34,35,36,38 Current language used in standards related to the built environment thus emphasizes physical safety through means of containment. In this way, the established standards and rules undermine, rather than promote, patient-centered care. Arguably counterproductive to safety, this lopsided focus applied in psychiatric settings likely increases the risk of interpersonal violence and harm to both patients and staff7,21,23,30 while creating a type of pervasive psychological harm to patients that is difficult to quantify.39
It seems clear that there is a need to consider raising the floor of acceptable standards for care quality in inpatient psychiatric settings. Standards for the built environment should align with both the empirical literature and society’s expressed value of patient-centered care. However, an argument against raising the baseline of standards is that there are trade-offs between quality and quantity. These trade-offs are not exclusive to inpatient psychiatry—they are widely discussed in inquiries concerning the sociology of mental health,40 physician labor supply,41 and public health services,42 among other topics—and there is even a journal called Quality & Quantity, in which some of the work on such trade-offs has appeared. But is this trade-off between quality and quantity relevant to inpatient psychiatry—in other words, will strengthening standards for the built environment lead to reductions in psychiatric beds, and are we faced with a bed shortage? Is access to anything better than nothing? We evaluate these concerns using empirical and ethical frameworks.
We begin by examining the current evidence for patient-centered standards causing a reduction in bed supply. A consequentialist ethical framework positions us to evaluate actions in terms of their consequences and is one approach to evaluating trade-offs (eg, between access to and quality of care43) posed by updates to standards that result in reduced bed supply. A consequentialist might ask, “What is the evidence that the adoption of patient-centered standards will result in a reduction of psychiatric beds?” There is no evidence to suggest that adoption of patient-centered standards for the built environment would reduce psychiatric beds. One can look to the Centers for Medicare and Medicaid Services’ Inpatient Psychiatric Facility Quality Reporting Program (IPFQR) as the most proximal comparison in terms of time, place (United States), and orientation towards quality.44,45
The IPFQR is a national quality measurement and reporting program that attempts to hold facilities accountable on metrics related to baseline standards of care treatment. While it has included some structural measures of quality (eg, presence of electronic health information exchange, measurement of patient experience44), the program currently focuses primarily on care process (eg, care coordination, screening for metabolic conditions) and utilization outcomes (eg, follow-up visits, readmission rates).46 Since the program was implemented in the last quarter of 2012, there were no observed reductions in psychiatric beds.47 In fact, over the years, a growing share of inpatient psychiatric beds are now owned by large for-profit companies, with new construction and continued investment projected for the future.47 That these beds are increasingly owned by profit-maximizing firms48,49 is a concerning trend, further emphasizing the need to strengthen our accountability mechanisms and direct attention to quality of care. However, the evidence does not support a narrative that improving quality standards will reduce access to psychiatric beds.
Furthermore, the fact that the built environment is a fixed feature of a facility and does not vary based on patient characteristics reduces the likelihood that a facility would face perverse incentives to cherry-pick more desirable patients and thereby reduce access. By contrast, process and outcomes standards, such as restraint use and readmission rates, might incentivize facilities to cherry-pick patients they expect will help them perform better on those standards, thus limiting access to certain patient groups.50
Moreover, even if the standards outlined structural requirements that could only be addressed through a change in space and occupancy, details of the implementation of these standards—or the specific regulatory rules, incentives, and supports—would likely moderate the degree of fidelity that hospitals would be compelled to meet. For example, existing facilities could be “grandfathered” in when faced with certain mandates, such that the formal rules of the fixed architecture of buildings would primarily apply to new builds (the approach taken by the Americans with Disabilities Act).51 Thus, improved standards for the built environment are unlikely to lead to cherry-picking of patients or reduction of beds, and the operationalization of standards and specific regulatory rules, incentives, and supports can mitigate reductions in access.
What is the ethical justification for updating standards even if doing so reduces psychiatric bed supply? Consequentialism is centrally concerned with the utility, or consequences, of actions.39 Under this framework, revising standards might be unethical if, overall, it reduced access to beneficial care (or the amount of “happiness” across persons). In order for this cause-effect relationship to hold, there would, firstly, need to be a reduction in access to inpatient psychiatric care directly attributable to the revision of standards. Secondly, the care that would have existed absent the revision of standards would have to have had a net benefit to most of those patients in the counterfactual world. We have previously disposed of the first proposition. As for the second, the justification for more psychiatric beds is that greater availability of beds promotes the well-being of individuals and society. This is a problematic assumption for several reasons.
First, a bed is a venue of care, not a type of care. For the past 5 decades, the thrust of US mental health policy has been on attempting to deliver high-quality care in alternate venues, (ie, in ambulatory settings); such initiatives included attempts to expand access to community mental health care under the Kennedy Administration.52 This shift is also reflected in the Olmstead v LC Supreme Court decision, which mandated community services for people with disabilities, including those with serious mental illness, and clarified that needless institutionalization of psychiatric patients is discrimination.53,54 Scholars working on the ethics of alternatives to hospitalizations have proposed, for example, that objective consequentialism be used to justify care in least restrictive environments.55
Second, access to any bed, regardless of its quality, could cause more harm than benefit.11 Recognition of this fact is why civil commitment processes operate under close judicial scrutiny and are designed to ensure that hospitalization is used for protective or therapeutic rather than for custodial purposes.56 Indeed, empirical evidence demonstrates that patients’ experiences of patient-centered care while hospitalized are related to outcomes; those discharged from facilities rated poorly for patient-centered care were more likely than those discharged from highly rated facilities to experience negative outcomes, such as a reduction in trust and willingness to engage in care.25
Third, the effectiveness of inpatient psychiatry as a population-level intervention to prevent suicide and improve outcomes lacks evidence, despite its effectiveness for both suicidal and nonsuicidal patients having been studied since the 1950s.57,58,59,60,61 In fact, suicide rates have increased by about 30% since 2000,62 with the risk of suicide being about 300 and 200 times the general global rate within the first week and month of discharge from inpatient psychiatry, respectively.63,64 Experts have questioned if some of this increased suicide risk is due to iatrogenic harm of inpatient psychiatric care (eg, experiences of dehumanization and hopelessness) rather than being attributable entirely to patient selection or external factors in patients’ personal lives.65
Finally, bed availability is not synonymous with access. Indeed, emergency department boarding of psychiatric patients is related to inpatient facilities’ preference for more “desirable” patients (eg, those who are easier to manage and place postdischarge and who have desirable insurance)66 and the difficulty in making beds available through discharging clinically ready patients due to a lack of community-based services.67
A calculus here is which treatments, delivered in which settings, best promote which individuals’ recovery. Bed availability is one of several possible elements, not the sole element of recovery. Our empirical analysis suggests that improving standards for the built environment will not reduce bed availability, and our ethical analysis suggests that even if such reductions occur, they might not be entirely undesirable. Consequently, the default conclusion is to revise standards for the built environment to align with patient-centered care. Raising the floor on care quality will likely lead to greater net benefit than if we were to continue to accept the status quo.
Current national standards for the built environment applied to inpatient psychiatric care do not appropriately reflect the empirical literature or society’s value of patient-centered care. Based on our empirical and ethical analysis, we have concluded that there is a need to improve standards for the built environment to better reflect society’s value of patient-centered care, even in a world where updating standards would cause a reduction in beds, though this scenario is unlikely.
Focusing on the current system’s capacity, which lacks evidence of its utility to patients and communities, prevents the type of disruption needed for a more patient-centered treatment system.7 Improved standards would provide the foundation needed to support implementation of patient-centered built environments. Moreover, some actions can be taken by implementers of standards to mitigate, monitor, and address unintended consequences of implementation in ways that respect the spectrum and nuance of the care needs of a diverse patient population as well as the operationalization of patient-centered care.
Gose J. As mental health crisis grows, more doors open to care. New York Times. April 11, 2023. Accessed October 13, 2023. https://www.nytimes.com/2023/04/11/business/mental-health-addiction-care.html
Tyrer P, Sharfstein S, O’Reilly R, Allison S, Bastiampillai T. Psychiatric hospital beds: an Orwellian crisis. Lancet. 2017;389(10067):363.
Marino P. A lack of psychiatric treatment beds in California puts an enormous strain on patients, staff and the community. Monterey County Weekly. April 6, 2023. Accessed October 6, 2023. https://www.montereycountyweekly.com/news/cover/a-lack-of-psychiatric-treatment-beds-in-california-puts-an-enormous-strain-on-patients-staff/article_11efdca0-d49f-11ed-98ca-e33650a1468a.html#:~:text=THE%20NEED%20FOR%20PSYCHIATRIC%20BEDS,acute%20beds%20for%20longer%20stays
Shields MC, Beidas RS. The need to prioritize patient-centered care in inpatient psychiatry as a matter of social justice. JAMA Health Forum. 2022;3(2):e214461.
Gallagher M, Perlin ML. “The pain I rise above”: how international human rights can best realize the needs of persons with trauma-related mental disabilities. Fla J Int Law. 2018;29:271-301.
Beers CW. A Mind That Found Itself. Longmans, Green & Co; 1917.
Bly N. Ten Days in a Mad-House: Nellie Bly’s Experience on Blackwell’s Island—Feigning Insanity in Order to Reveal Asylum Orders. Cosimo Classics; 1905.
Shields MC, Hollander MAG. Complaints, restraint, and seclusion in Massachusetts inpatient psychiatric facilities, 2008-2018. J Patient Exp. 2023;10:23743735231179072.
Institute of Medicine. Crossing the Quality Chasm: A New Health System for the 21st Century. National Academy Press; 2001.
Huckshorn KA. Six core strategies for reducing seclusion and restraint use©. National Association of State Mental Health Program Directors. Revised 2008. Accessed October 13, 2023. https://www.nasmhpd.org/sites/default/files/Consolidated%20Six%20Core%20Strategies%20Document.pdf
Bowers L, James K, Quirk A, Simpson A, Stewart D, Hodsoll J; SUGAR. Reducing conflict and containment rates on acute psychiatric wards: the Safewards cluster randomised controlled trial. Int J Nurs Stud. 2015;52(9):1412-1422.
Shields MC, Hollander MAG, Busch A, Kantawala Z, Rosenthal M. Patient-centered inpatient psychiatry is associated with outcomes, ownership, and national quality measures. Health Aff Sch. 2023;1(1):qxad017.
Shepley MM, Pasha S, Ferguson P, Huffcut JC, Kiyokawa G, Martere J. Design research and behavioral health facilities. Center for Health Design; 2013.
US Department of Veterans Affairs. Design Guide for Inpatient Mental Health and Residential Rehabilitation Treatment Program Facilities. US Department of Veterans Affairs; 2021. Accessed December 3, 2023. https://www.cfm.va.gov/til/dGuide/dgMH.pdf
Carr RF. Psychiatric facility. Whole Building Design Guide. Updated April 7, 2017. Accessed August 27, 2023. https://www.wbdg.org/building-types/health-care-facilities/psychiatric-facility
Office of Construction and Facilities Management. Design Guide: Mental Health Facilities. US Department of Veterans Affairs; 2017. Accessed August 17, 2023. https://www.wbdg.org/FFC/VA/VADEGUID/ARCHIVE/dgmh_2010_Rev2017.pdf
Frierson RL. Inpatient treatment. In: Gold LH, Frierson RL, eds. The American Psychiatric Association Publishing Textbook of Suicide Risk Assessment and Management. American Psychiatric Association Publishing; 2020:chap 16.
Clinical practice guidelines. American Psychiatric Association. Accessed August 27, 2023. https://www.psychiatry.org/psychiatrists/practice/clinical-practice-guidelines
Workgroup of the Committee on Professional Practice and Standards; Board of Professional Affairs. APA guidelines on evidence-based psychological practice in health care. American Psychological Association; 2021. Accessed October 17, 2023. https://www.apa.org/about/policy/psychological-practice-health-care.pdf
NFPA 101®: Life Safety Code®. National Fire Protection Association; 2015.
Health care/CMS. National Fire Protection Association. Accessed August 27, 2023. https://www.nfpa.org/Codes-and-Standards/Resources/Standards-in-action/NFPA-resources-for-CMS-requirements-on-NFPA-99-and-NFPA-101
Joint Commission. R3 report: requirement, rationale, reference. The Joint Commission; 2018. Updated May 6, 2019. Accessed January 19, 2024. https://www.jointcommission.org/-/media/tjc/documents/resources/patient-safety-topics/suicide-prevention/r3_18_suicide_prevention_hap_bhc_5_6_19_rev5.pdf?db=web&hash=887186D9530F7BB8E30C28FE352B5B8C#:~:text=These%20new%20requirements%20are%20at,as%20high%20risk%20for%20suicide
Quality, safety and oversight—certification and compliance. Centers for Medicare and Medicaid Services. Updated October 6, 2023. Accessed October 17, 2023. https://www.cms.gov/medicare/health-safety-standards/certification-compliance
Plaisier I, Beekman AT, de Bruijn JG, et al. The effect of social roles on mental health: a matter of quantity or quality? J Affect Disord. 2008;111(2-3):261-270.
Fortin B, Jacquemet N, Shearer B. Policy analysis in the health-services market: accounting for quality and quantity. Ann Econ Stat. 2008(91-92):293-319.
Munson R. Intervention and Reflection: Basic Issues in Bioethics. Cengage Learning; 2013.
Medicare program; FY 2024 inpatient psychiatric facilities prospective payment system-rate update. Fed Regist. 2023;88(68):21238-21314.
Salyer S. 3 companies vie for mental health business. Herald Net. June 29, 2014. Accessed October 31, 2023. https://www.heraldnet.com/news/3-companies-vie-for-mental-health-business/
Kowalczyk, L. Families trusted this hospital chain to care for their relatives. It systematically failed them. Boston Globe. June 10, 2017. Accessed December 9, 2017. https://www.bostonglobe.com/metro/2017/06/10/arbour/AcXKAWbi6WLj8bwGBS2GFJ/story.html
Humbyrd CJ. The ethics of bundled payments in total joint replacement: “cherry picking” and “lemon dropping.” J Clin Ethics. 2018;29(1):62-68.
DiPolito SA. Olmstead v LC—deinstitutionalization and community integration: an awakening of the nation’s conscience? Mercer Law Rev. 2006;58(4):1381-1410.
Marshall M, Crowther R, Sledge WH, Rathbone J, Soares‐Weiser K. Day hospital versus admission for acute psychiatric disorders. Cochrane Database Syst Rev. 2011;2011(12):CD004026.
Garnett MF, Curtin SC, Stone DM. Suicide mortality in the United States, 2000-2020. NCHS data brief 433. US Department of Health and Human Services; 2022. Accessed October 17, 2023. https://www.cdc.gov/nchs/data/databriefs/db433.pdf
Chung D, Hadzi-Pavlovic D, Wang M, Swaraj S, Olfson M, Large M. Meta-analysis of suicide rates in the first week and the first month after psychiatric hospitalisation. BMJ Open. 2019;9(3):e023883.
Kraft CM, Morea P, Teresi B, et al. Characteristics, clinical care, and disposition barriers for mental health patients boarding in the emergency department. Am J Emerg Med. 2021;46:550-555.
McBain RK, Cantor JH, Eberhart NK, Huilgol SS, Estrada-Darley I. Adult psychiatric bed capacity, need, and shortage estimates in California—2021. RAND Corporation; 2022. Accessed October 17, 2023. https://www.rand.org/pubs/research_reports/RRA1824-1-v2.html



