Policy Forum
Dec 2024
Peer-Reviewed

Internationally, there is a long history of improving dementia care quality by focusing on patients’ strengths and supporting environments that normalize their daily routines. The European dementia village is a pioneering health care site: 4 acres of integrated housing and amenities that include large exterior walkways around gardens, restaurants, and shops. A US-based conceptual model is the dementia friendly city center, which integrates health care service delivery into adaptive reuse and urban revitalization. This article discusses how these models envision structures and spaces of caregiving and habitation.
It is estimated that more than 5 million Americans have some form of dementia.1 As the population of North Americans 65 years and older is projected to grow from 54 million in 2015 to 95 million by 2050,2 so, too, will the numbers of new cases of dementia.1
Neuropsychiatric symptoms in individuals with dementia are heterogeneous and largely unpredictable, affecting emotional experience, thought content, perception, and motor function.3 People living with dementia might need help with their daily activities while making the most of their present strengths.4 This manuscript addresses the ethics of past and future memory care models, with a specific focus on the existing European dementia village (DV) model and a newly proposed model, both of which negotiate risk and autonomy in decision sharing and decision-making.
Historically, the experience of living with dementia can be overwhelming for individuals and their families without appropriate support. Once family caregivers no longer feel competent in their caregiving role, an individual with dementia might be institutionalized, leading to negative outcomes, including a feeling of disconnection from home, family, community, and meaningful activities.5 Meaningful activities in particular can stimulate a sense of well-being and personal fulfillment and promote both physical and mental health—in essence, by creating daily meaning. Although it is imperative that vulnerable populations be provided care settings that allow for personal fulfillment, traditional medical models of memory care engender a sense of isolation and depression in residents through the organizational culture and physical layout of the setting. This biomedical approach to care focuses on symptoms and on social distance between residents and staff, with the requirements of organized routines trumping residents’ personal preferences. As has been written elsewhere, “these environments are institutional in design and size, with little access to outdoor spaces” due to lack of adequate and safe adjacent space for walking, gardening, and other outdoor activities.6
Barrett et al describe a holistic approach to memory care in which the impacts of multiple dimensions of the built environment on the well-being of people living with dementia are individually targeted in specific environments.4 This emphasis on multidimensionality captures how people experience the built environment in daily life—not as discrete environmental elements but as those elements combined. In particular, Barrett et al suggest an individual’s baseline capacity “can be augmented by a combination of the empowerment provided by the physical/technological environment, the support of the caring/social environment” and treatment through medical means.4 The importance of these environments to well-being is demonstrated by Zimmerman et al, who found that, in nursing homes, the physical environment of the facility (poor environmental quality) and the social environment of the facility (lack of privacy, low visitation rates) were associated with high rates of hospitalization for infection.7
Autonomy is seen as an overarching problem, not only because institutions limit residents’ freedom, but also because the existential conditions that create the need for long-term care undermine autonomy conceived of as independent self-sufficiency by bioethicists.8 Filling the gap between “ideal” autonomy and dependency is crucial if the holistic approach to the built environment set out above is to be operationalized. Dementia care stakeholders, therefore, face a range of daunting environmental and ethical challenges in searching for improved models of care.9
Internationally, dementia friendly initiatives have been developed to support the creation of enabling environments that maximize independence for individuals living with dementia through collaboration with diverse community stakeholders.10 Originally termed Dementia Friendly Communities in England, these communities are often cities, towns, or villages where a concerted effort is made to educate citizens about dementia so that those living with the disease are understood, respected, and supported. In addition, dementia-friendly environments are deeply rooted in design efforts that center on the fulfillment of very basic human needs. With that said, environments for people with dementia do not have a fundamentally different appearance from other environments.11 A growing number of cities and communities are implementing dementia friendly initiatives with stakeholder advocacy, which requires sharing of ideas between networks of people representative of the local community and involving people affected by dementia.12
Addressing the challenges of improved dementia care settings requires attention to the ethics of past and future care models and, in particular, the European DV model. The first of these model villages opened on 4 acres in 2009 in the Netherlands. Since then, the model has been successfully repeated in other countries.13
The first DV, Hogeweyk, has been operated with the intention of humanizing care while providing a normal life to residents. It is designed as a traditional Dutch neighborhood, with opportunities for residents to wander freely while taking part in programs and activities throughout the village, such as shopping at supermarkets and dining at restaurants and cafes.14 Purposefully designed to maximize resident autonomy while still minimizing safety concerns, the site is laid out around the outdoor areas with one primary outside entrance. The outdoor area includes gardens, seating, and bike paths designed by landscape architects who designed several different unique courtyards for residents’ walking experiences.15 Figures 1 and 2 show the principle public spaces, including the supermarket and outdoor walkway with a café and bar.
Figure 1. Dementia Village Public Space

Reproduced with permission of Sage © 2023 from Roberts.6
Figure 2. Dementia Village Walkway

Reproduced with permission of Sage © 2023 from Roberts.6
The village model is organized in such a way that personal care is integrated into daily routines, with 6 to 8 residents living in each of the 23 households. Each household has its own kitchen, living and dining room, and individual resident bedrooms with attached bathrooms. In addition, rather than the traditional staff hierarchy in which tasks are divided among specific care staff (eg, cooking and cleaning staff, certified nursing assistants for bathing and dressing), care staff in the household model work in one household only and conduct most tasks of daily living as a universal worker. The universal care team organizes the shopping, cooking, and laundry within each household, while residents give input on what meals they want and when to eat them and are encouraged to help out with chores.13
Previous studies have shown that staff working within a universal model of care experience more job satisfaction, higher motivation, and less burnout than staff working in traditional care settings.16 This finding is important, because as staff become engaged in their universal duties of care, cooking, and cleaning in their household, they often acquire a sense of empowerment, resulting in lower turnover rates. In addition, as care staff get to know residents more deeply, they are better able to observe changes in individuals’ physical and mental health.16
To date, there have been no developments in the United States on the scale of the Hogeweyk Dementia Village, as providers may not have the appropriately sized property to offer multiple activities and advanced medical services for residents or the funding to develop them.13 Providers are also concerned about the bottom-line costs associated with new construction of a care setting this size. One solution to the perennial challenges faced by providers, planners, and designers is to think more creatively: How do we design with what we have?
Referring to the DV model as a precedent, the author and a research team at a Midwestern university began to look for new ways of addressing the needs of those living with dementia in their community.13 In searching for innovative options, repurposing existing structures—in particular, vacant urban malls—was identified as an option for the large sites needed for the European model of DVs. These settings were identified as dementia friendly city centers (DFCCs).
A working group of stakeholders in health care, design, and development identified several closed mall sites that could align with community needs with respect to location, size, and layout and decided on a permanently closed 800 000 square foot mall to serve as a case study site for initial DFCC conceptual designs. Figure 3 shows the DFCC case study site and conceptual site plan. Figure 4 shows a birds-eye view of the existing mall and the 3-D rendered model of the DFCC from a similar vantage point.
Figure 3. Existing Closed Mall Site and Proposed DFCC Adaptive Reuse Site Plan
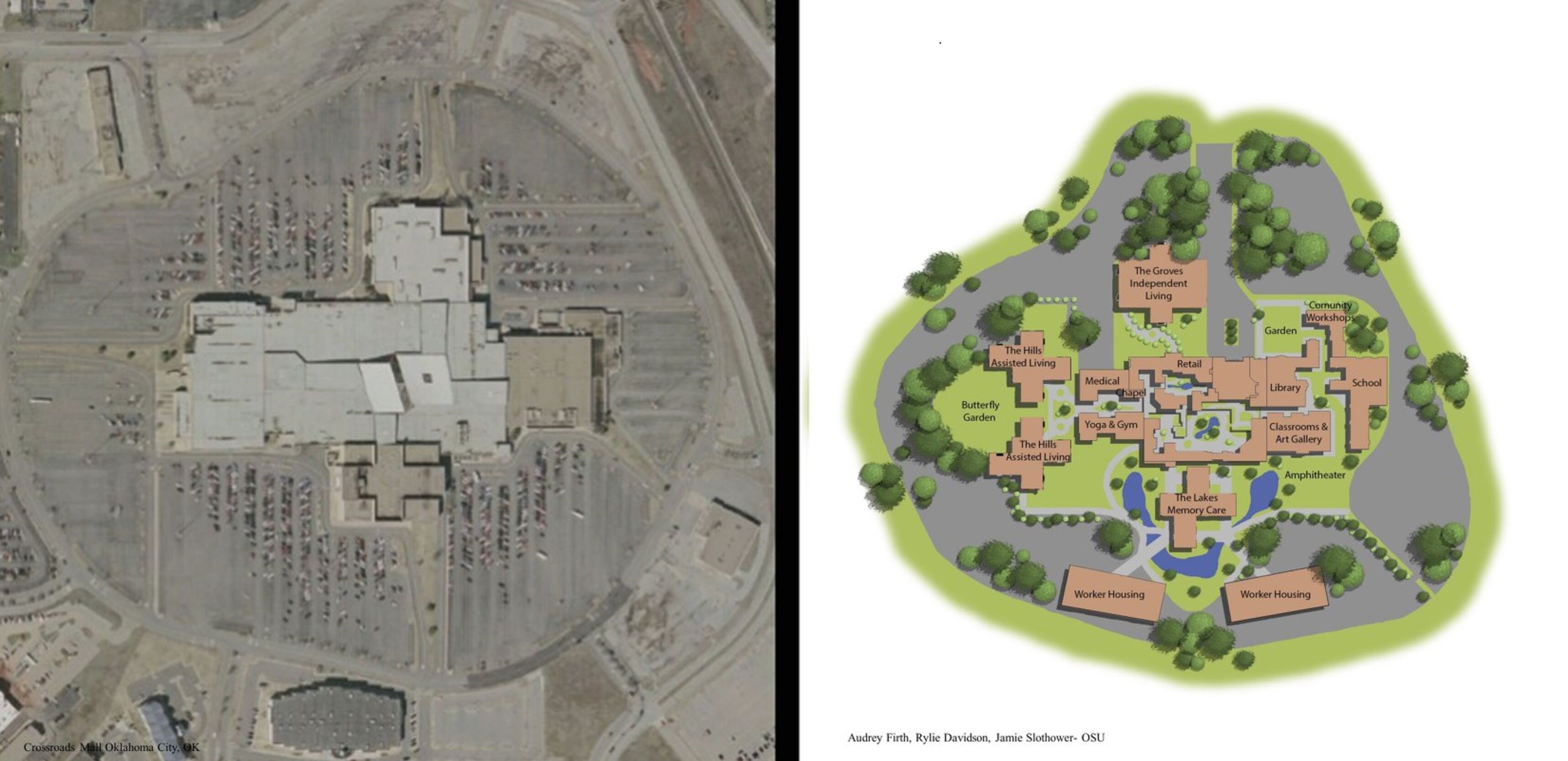
Reproduced with permission of Sage © 2021 from Roberts and Shehadeh.13
Figure 4. Birds-Eye View of Existing Mall and Proposed DFCC Services and Attached Housing

Reproduced with permission of Sage © 2021 from Roberts and Shehadeh.13
Through several community workshops and focus groups, 3 key topics were developed and addressed, along with the development of conceptual designs.14 Figures 5 and 6 show the designed DFCC central courtyard and a typical outdoor walkway.
Figure 5. Proposed DFCC Central Courtyard
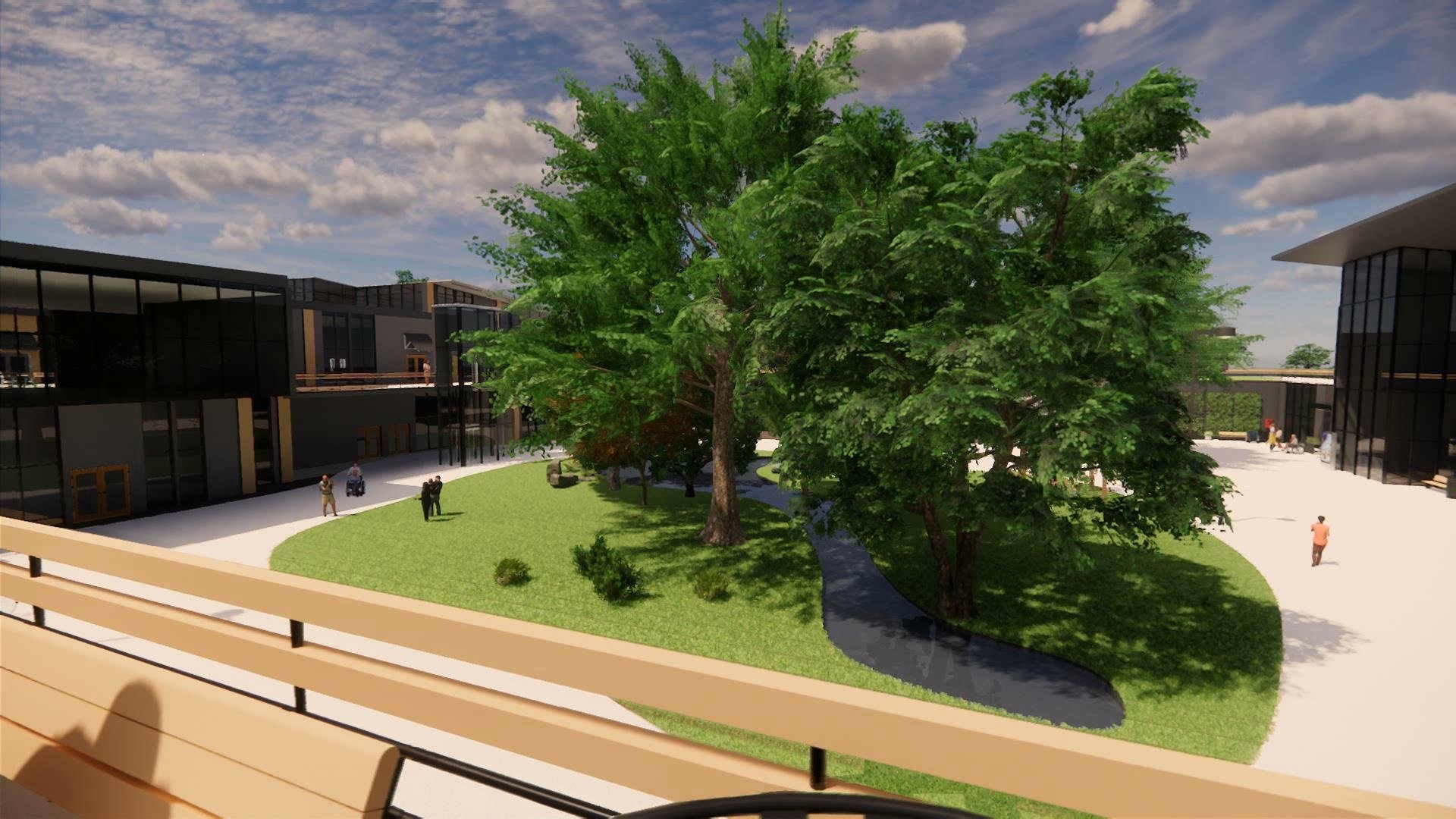
Photo courtesy of Emily Roberts.
Figure 6. Proposed DFCC Exterior Walkway

Photo courtesy of Emily Roberts.
Organizational factors. Adaptive reuse is taking place in mall sites around the United States for education and health care. Being able to convert malls for uses appropriate for individuals living with dementia can be seen as an opportunity but also as a challenge. Several key organizational factors are necessary to create a viable city center solution, including wayfinding elements—such as landmark clocks, sculptures, and signage—and universal design elements that allow of ease of use, such as ramps, unobstructed entryways, and interior spaces. A principal advantage of adaptive reuse is sustainability, in that a large structure is not being demolished with tons of debris being placed in a landfill. The building is being saved, and there is an energy cost savings of not having to produce bricks or steel for new construction. The infrastructure is all there in a closed mall site, with structural elements that allow designers to take away and build back in flexible configurations.14
Onsite amenities. The DFCC case study designs include an integrated medical complex that can provide general medical care for both onsite residents and the general public. Also included is a “supermarket, library, full-service restaurant, and several outdoor areas for eating and socializing.”13 Pedestrian walkways connect adjacent housing, and the removal of several sections of the existing roof provides large internal courtyards. Three levels of purpose-built housing are proposed, “including independent living apartments for caregiver/care recipient dyads, assisted living, and 24/7 memory care.”13
Public-private partnerships. Many types of innovative public-private partnerships can be created within the DFCC care model for fiscal viability. A development corporation or group of owners can take on the adaptive reuse of the mall and lease the converted space to a medical provider, adult day center, or public institutions such as libraries, community workshops, or education centers. The partnership can create income from amenities, and, in turn, multiple providers can proceed with the development of adjacent purpose-built independent living, assisted living, and 24/7 memory care housing.14
The current moment in time could be propitious for innovative change in dementia care in the United States through models like the DFCC. Malls around the country are struggling, and mall owners are becoming more responsive to community needs.17 The proposed mixed-use pallet in the DFCC creates a city center with living environments and amenities, potentially raising the value of economically distressed properties and communities. And, perhaps most importantly, resident proximity to outdoor amenities allows for socialization, meaningful activities, and sensory stimulation that encourage engagement with community members and confer psychological and physical as well as social benefits. What happens outside of the home—where one can explore and socialize—is perhaps the most distinct and powerful benefit of the existing village and proposed city center models.
In the United States, where the standard memory care environment is restrictive, the DFCC concept allows for flexibility of programming and spaces that fit the needs of many residents’ lifestyles and personal styles of engagement. Some residents enter the environment wanting to be in the middle of the action, while others prefer to be in a more private setting that can give them the opportunity to see what is going on before deciding if they want to participate. That ability for choice and autonomy in how one spends one’s day is central to the ethics of dementia care. In addition, the flexibility of the housing types in the DFCC allows intergenerational residents as well as spouses to live together. In essence, the DFCC can be seen as a form of respite for the caregiving spouse living in an independent living apartment, as it allows the caregiver to step outside of that role whenever they wish without guilt or concern about whether their spouse will be in a safe and secure environment. Being able to go to work or a class or just run errands allows the caregiving spouse to maintain the normalcy of life that prevailed before the spouse’s dementia diagnosis.
Finally, due to the size of the repurposed malls in the DFCC model, there is the opportunity to align the DFCC with a university or teaching hospital to bring in students for practicums who would help with the day-to-day operations within the city center. This initiative, as well as volunteerism within the larger community, will play an important role in the ability of residents to remain autonomous while having support available when and where they need it.
Separately and together, we can work to deliver new interventions that can make a difference for those living with dementia and their families. The village and city center care models provide an ethical roadmap for the future by not only addressing well-being of residents, but also taking on larger, more global issues such as sustainable building practices, regreening urban landscapes, and their economic impact. Further exploration of the DFCC model is required to address possible financial and regulatory constraints that accompany the development of necessary public health infrastructure.
The impact of social isolation in our current care system must be weighed against the frequent overregulation of the daily movements of those living with dementia. Viewing individuals with dementia as patients who must be kept safe at all costs is not realistic. According to our cultural norms, if you age without a diagnosis of dementia, then you can live life taking any risk that you want—you can go skydiving (think former President George H. W. Bush). But if you have a dementia diagnosis, often it might seem that everything stops around you. This might be many communities’ biggest ethical challenge: to see people living with dementia not as patients but simply as people who have a set of needs requiring different types of support to live with those needs.
Often it is problematic to introduce an innovative idea without an understandable precedent or prototype. Identifying precedents like the DV model in Europe and thinking outside of the box with proposed models like the DFCC here in the United States can begin to motivate new ways of thinking about memory care environments. It is imperative that, as a society, we turn from paternalism to inclusivity in dementia care policy. From the inception of the first DV in 2009,6 there was a shared vision and mutual understanding of goals among its founders and architects. The proposed DFCC is more than simply a physical location; it is an inclusive community designed to meet the special requirements of people living with dementia and their spouses, while at the same time creating a desirable living environment for those with or without dementia.
Clinicians and designers are beginning to understand that current and future generations of older adults will not accept living in an environment in which they do not have choices in how to spend their days. So, ask yourself the question, What options would I like to see in my future environment, with or without dementia? Thus begins the conversation about the ethics of dementia care.
Olivari BS, French ME, McGuire LC. The public health road map to respond to the growing dementia crisis. Innov Aging. 2020;4(1):igz043.
He W, Goodkind D, Kowal P; US Census Bureau. An Aging World: 2015. US Government Printing Office; 2016. International Population Reports P95/16-1. Accessed December 13, 2023. https://www.census.gov/content/dam/Census/library/publications/2016/demo/p95-16-1.pdf
Cerejeira J, Lagarto L, Mukaetova-Ladinska EB. Behavioral and psychological symptoms of dementia. Front Neurol. 2012;3:73.
Roberts E. A conversation about the ethics of past and future memory care models: perspectives from the first two European dementia villages. Inquiry. 2023;60:469580221150565.
Agich G. Dependence and Autonomy in Old Age: An Ethical Framework for Long-Term Care. Cambridge University Press; 2003.
Turner N, Morken L. Better Together: A Comparative Analysis of Age-Friendly and Dementia Friendly Communities. AARP International Affairs; 2016. Accessed September 5, 2024. https://www.aarp.org/content/dam/aarp/livable-communities/livable-documents/documents-2016/Better-Together-Research-Report.pdf
Marquardt G, Bueter K. Extending the continuum of care of people with dementia: building resilience. In: Ferdous F, Roberts E, eds. (Re)designing the Continuum of Care for Older Adults: The Future of Long-Term Care Settings. Springer; 2023:217-236.
Roberts E, Shehadeh A. Community visioning for innovation in integrated dementia care: stakeholder focus group outcomes. J Prim Care Community Health. 2021;12:21501327211042791.
Archer D. Stepping back in time: help for Alzheimer’s. Psychology Today. April 12, 2012. Accessed December 16, 2023. https://www.psychologytoday.com/us/blog/reading-between-the-headlines/201204/stepping-back-in-time-help-alzheimers
Roberts E, Carter HC. Making the case for centralized dementia care through adaptive reuse in the time of COVID-19. Inquiry. 2020;57:46958020969305.
Baily H. How to save a dying mall? Try moving in. ctpost. January 16, 2022. Accessed July 22, 2024 https://www.ctpost.com/columnist/article/Hugh-Bailey-How-to-save-a-dying-mall-Try-moving-16776034.php



