History of Medicine
Dec 2024
Peer-Reviewed
Design is and always has been interventional and clinically relevant. Modern evidence-based designers’ lineage was prominently shaped between 1800 and 1970. This article investigates hospital designs during this period that were correlated with patients’ health outcomes and suggests how this history influenced our present-day understanding of evidence-based design.
It is a common assumption that evidence-based design (EBD)—“the process of basing decisions about the built environment on credible research to achieve the best possible outcomes”1—is a recent development kindled by Roger Ulrich’s 1984 study that documented that patients in rooms with a view of trees recovered more quickly and at higher rates than patients with a view of a brick wall.2 Attempts to situate EBD in a larger historical trajectory have noted Florence Nightingale’s work in the 1860s but mention few precursors.3,4,5 This narrative is like telling the history of aviation from the Wright brothers to commercial air travel with no intermediate steps; accordingly, this article aims to fill in a few key gaps. The examples of hospital designs from the 1800s to the 1970s presented in this article show that the use of evidence has been the norm, not the exception, in clinically influential hospital design decisions.
Early 19th century hospital design strategies based on evidence focused on preventing hospital-acquired infections. Medical theories of the time considered bad air as the cause of diseases, and hospital practitioners related morbidity and mortality outcomes in various hospitals (and even in individual hospital rooms) to the architectural features that influenced air quality and flow.6,7,8 In response, hospital designers developed buildings that provided pure air in specific volumes and flow patterns with the intent to reduce internal disease transfer.9
As ongoing research redefined what constituted “pure” or “healthy” air, the variables studied and the design solutions proposed evolved. By 1800, hospital designers emphasized providing a minimum air space around each patient and maximizing natural (ie, open window) air flow.10,11 Yet natural air flow was inconstant; it varied with weather conditions. To create a more constant air flow, industrialist, fire-proof construction advocate and inventor William Strutt designed the new Derbyshire General Infirmary building with a novel closed-window, ducted heating and ventilation system.12 By the 1820s, early American architect Charles Bulfinch included a similar system in the new Massachusetts General Hospital.13 In the 1850s, Dr John Watson, a ventilation-obsessed surgeon at the New York Hospital, advocated similar closed-window, ducted systems in renovations of existing hospital buildings and in new construction (see Figure 1).14
Figure 1. Foundation, Basement, Upper and Attic Floor Plans of South Building, New York Hospital
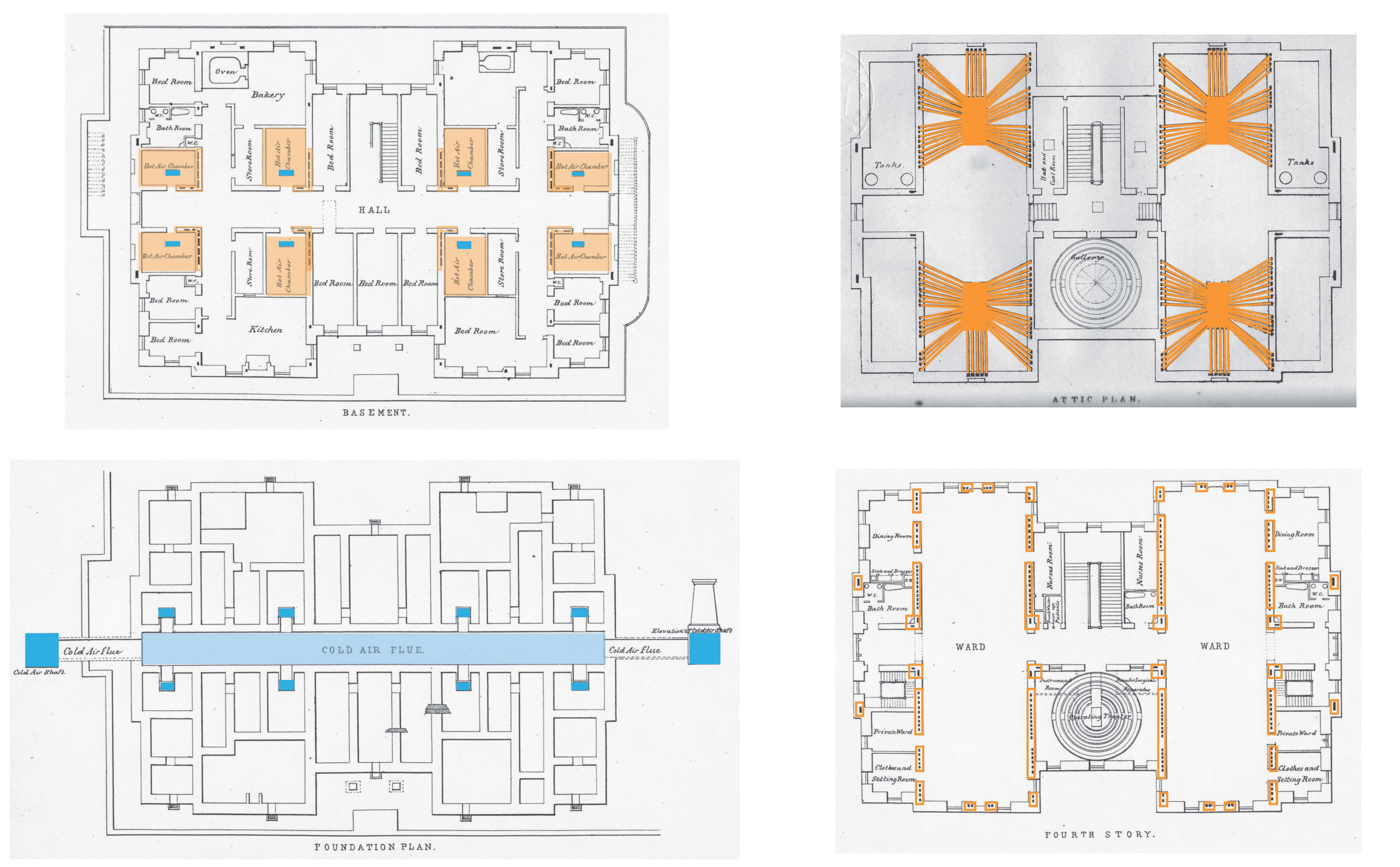
Reproduced from Smith JM. An address delivered on the occasion of the inauguration of the new South Building of the New York Hospital. ST Callahan & Co; 1855.
Figure shows cold air intake in basement (blue), hot air chambers in basement (light orange), ducts in walls on upper story (orange), and exhaust ducts in attic (orange).
By the 1850s, Florence Nightingale presented copious statistical evidence that patient outcomes in well-ventilated hospitals were vastly better than in poorly ventilated ones.15 Her “pavilion-ward” hospital design maximized open-window ventilation in a prescribed spatial relation to patient beds as a means of not only preventing airborne hospital-acquired infections but also improving outcomes through therapeutic exposure to fresh air (see Figure 2).9,16,17
Figure 2. Ideal Pavilion-Ward Plan
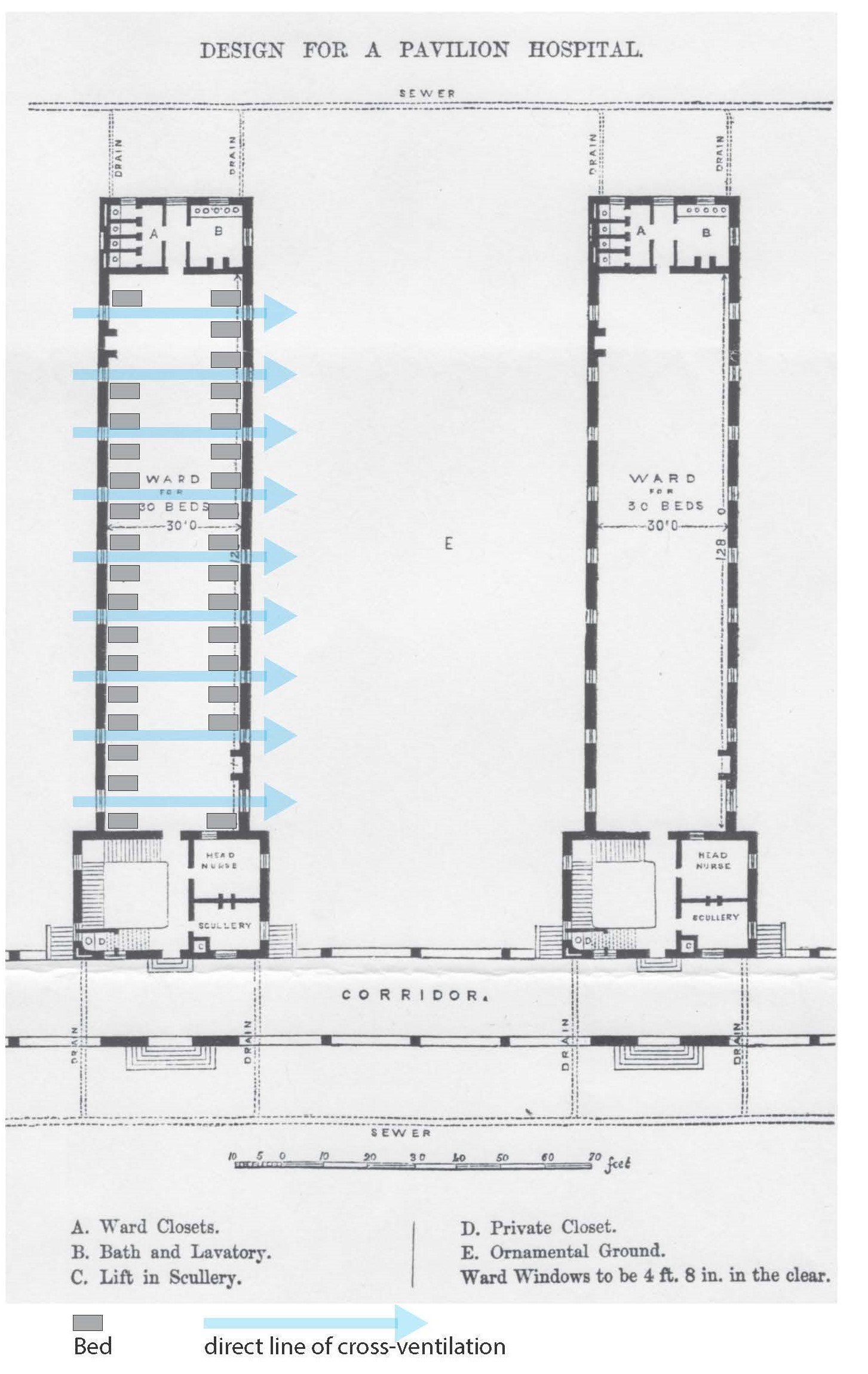
Reproduced from Nightingale F. Hospital construction. Wards. The Builder. 1858;16(816):641-643.
Figure shows window placement for maximum natural ventilation between beds, with graphic indications of beds and lines of window-to-window cross-ventilation added by author.
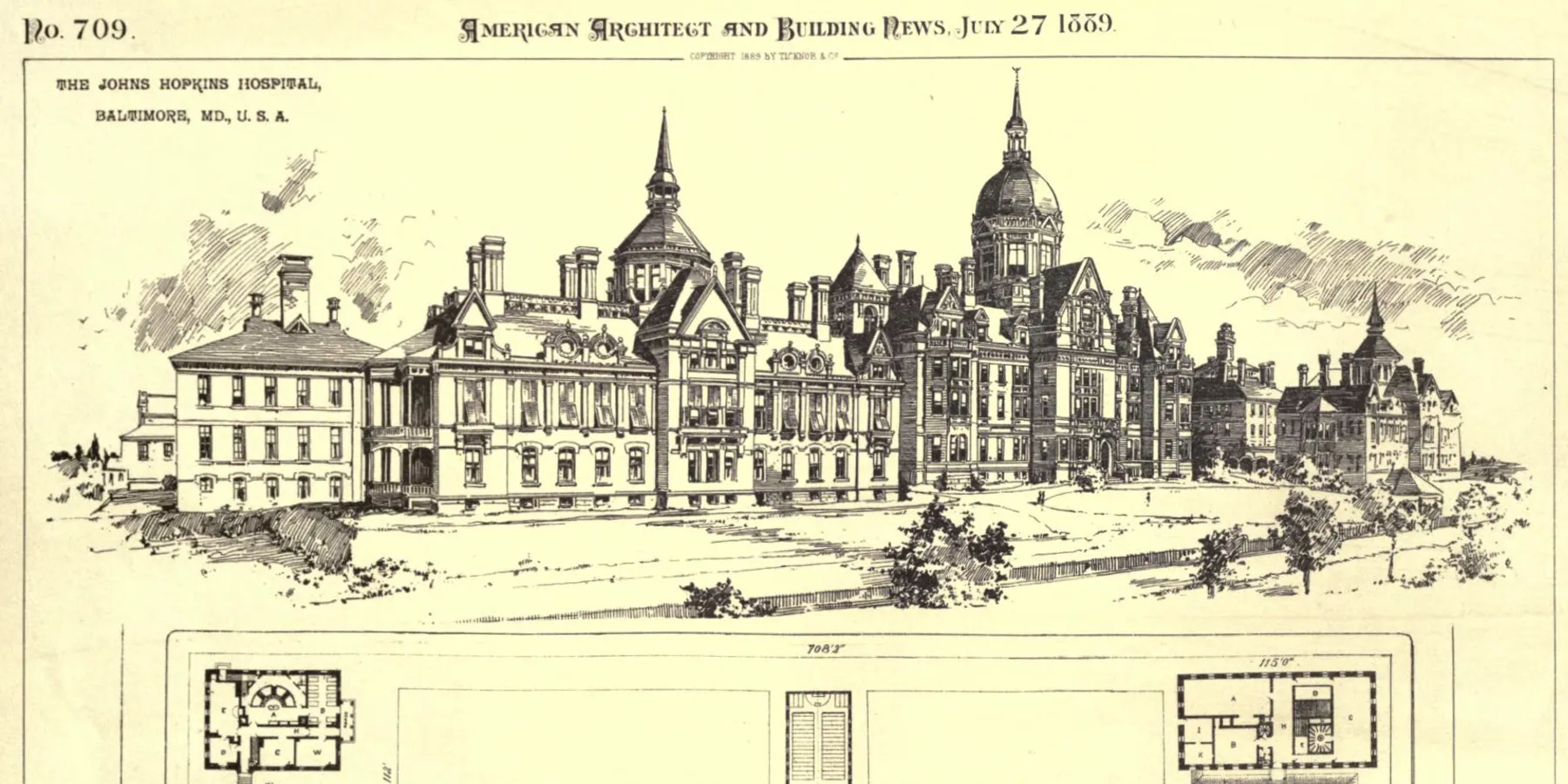
Early germ theory in the late 1860s provided evidence that dust-borne microbes caused disease; in response, hospital designers experimented with mechanically directed, closed-window ventilation systems that filtered out dust.18,19,20 In the 1870s, the board of governors of the newly endowed Johns Hopkins Hospital hired John Shaw Billings—a surgeon, Civil War military hospital doctor, and author of a postwar report on the healthiness of hospitals and barracks—to oversee the design of the new institution. Billings intentionally planned the new hospital facility as a “laboratory of heating and ventilation” with a variety of ward layouts and heating and ventilation system designs to provide data that would establish which ones yielded the best outcomes (see Figure 3).21,22,23
Figure 3. Plan of Johns Hopkins Hospital (Plate No. 709)
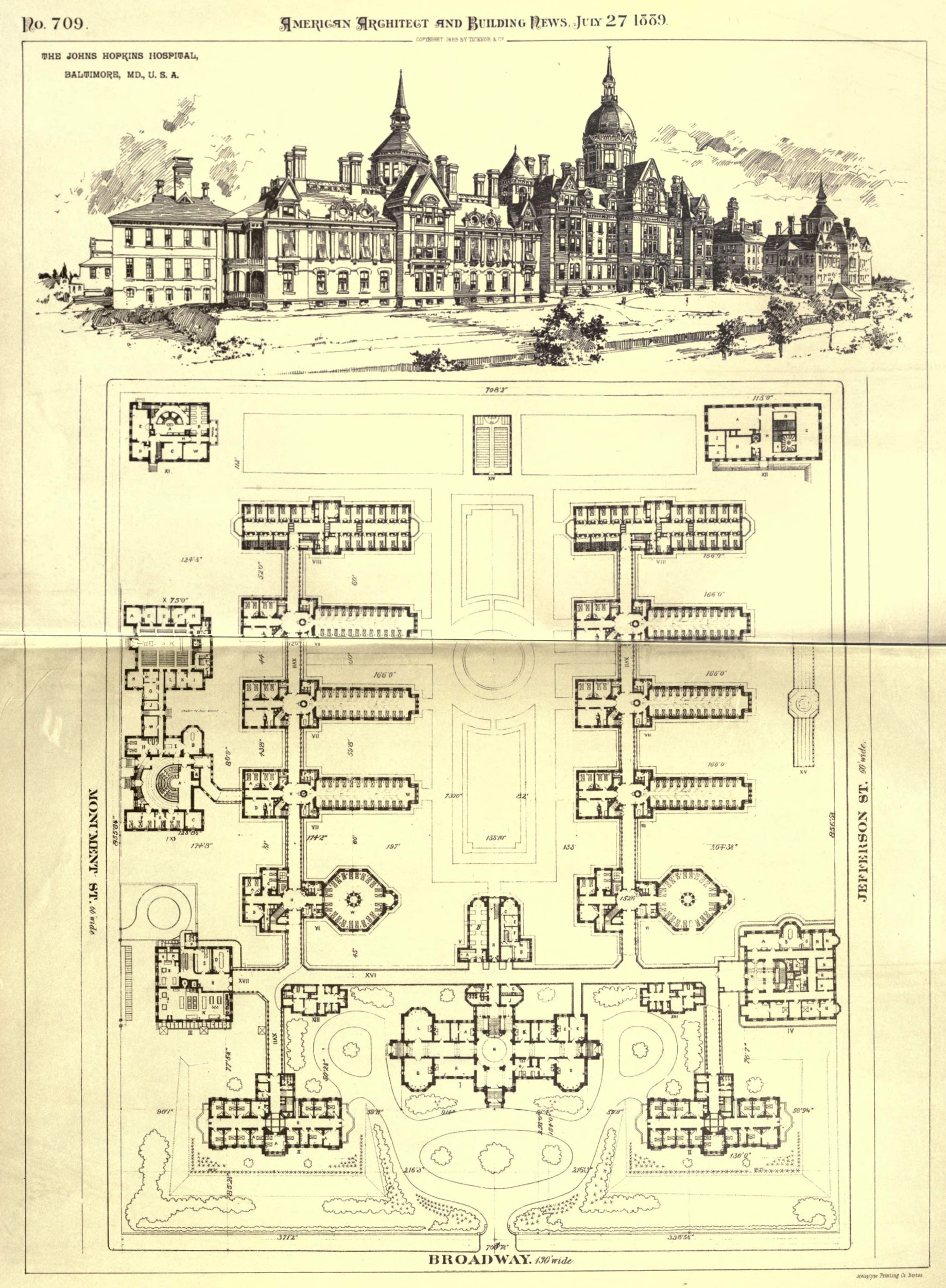
Reproduced from American Architect and Building News, 1889:26(709).
Patients were housed in octagonal wards, rectangular wards, and single-bed rooms in the isolation ward.
By the 20th century, increasing attention to direct contact as the means of spread of disease shifted attention from air to the interaction of design features and microbes. Designers of the Contagious Disease Unit of the Providence City Hospital in Rhode Island downplayed air flow and emphasized details that facilitated aseptic procedures (see Figure 4). Studies of materials, decontamination processes, functional details, and layouts that reduced the environmental microbial load and thereby minimized hospital-acquired infections continued for decades.24,25,26,27,28,29,30,31
Figure 4. Contagious Disease Buildings, Providence City Hospital
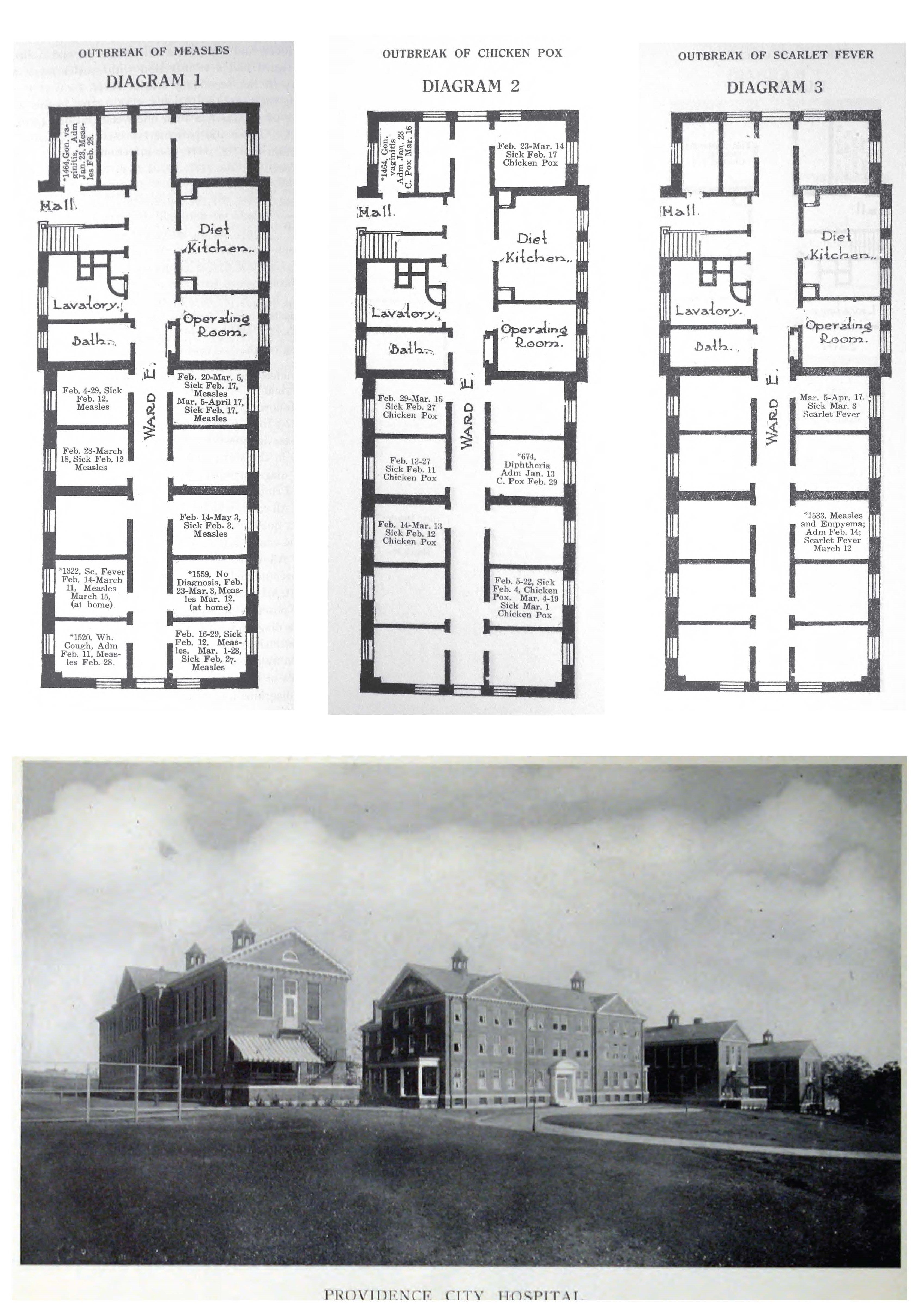
Reproduced from Annual Report of the Providence City Hospital (photo from 1910 issue, frontispiece; diagrams 1-3 from 1912 issue, pp. 38-40).
Based on extensive research by hospital supervisor D. L. Richardson and his collaborations with hospital architects, Martin & Hall, the Contagious Disease buildings (completed in 1911) were designed to limit contact infection and disregard air as a means of transmission. Active cases were assigned to doorless single-bed cubicles with extensive aseptic features to support aseptic barriered nursing techniques. In the first years of operation, all incidences of secondary infections were studied and mapped with the intent of determining if aerial infection was or was not a factor in transmission. Procedures and design details were changed in response to incidence.
Throughout the 19th and 20th centuries, publications did not keep pace with the rate of research and innovation, and designers undertook “study tours” to new and innovative hospital facilities to gather evidence for improved hospital designs.32 In the 1860s, surgeon and public health advocate Dr Stephen Smith and architect Carl Pfeiffer undertook an extended tour of hospitals in Europe and America prior to designing the new Roosevelt Hospital in New York City.33,34 Similarly, influential hospital architect Edward F. Stevens gained detailed knowledge of hospital operations and designs through his extensive travel to hospitals.35 Dr Christian R. Holmes, a physician and chair of the Board of Hospital Commissioners of Cincinnati General Hospital, determined the best design for the new model hospital facility after a travel study tour.36
Studies of therapeutic influences of specific environmental conditions and designs that realized those conditions blossomed in the 20th century.37 In 1906, prominent New York City physician Dr W. Gilman Thompson sent patients with a variety of diseases to a new, experimental rooftop “fresh air” ward and tracked their rates of improvement relative to those in the traditional enclosed wards.38,39 The widely publicized positive results encouraged hospitals across the country to add fresh air facilities.9,40
With the development of increasingly sophisticated mechanical ventilation systems that could humidify, cool or heat, and ventilate, studies examining the influence of “internal” controlled climate on patients also proliferated. By 1920, a geographer and advocate of the (now discredited) theory of environmental determinism, Ellsworth Huntington, demonstrated that air conditions in hospitals affected the postoperative death rate; this finding focused designer attention on providing the optimum environment for patients.41,42,43,44,45 Hospital practitioners built and assessed experimental “climate” or “weather” rooms in which the environmental conditions could be tailored to the exact therapeutic needs of a specific patient.46,47,48,49 Reports of unanticipated problems (eg, high humidity rooms for patients with breathing difficulties experienced condensation and mildew) and possible design solutions to those problems appeared alongside reports of clinical successes.50 After Boston Children’s Hospital pediatrician Kenneth D. Blackfan published a study in 1933 with public health engineer Constantin P. Yaglou and pediatric nurse Katherine MacKenzie Wyman showing that improved outcomes for premature infants were correlated with improved air conditioning, installation of air conditioning in nurseries became standard practice.51,52,53 In operating rooms, studies showed that air conditioning at the proper humidity balance made surgeons more comfortable, reduced condensation that could drip onto the operating field, and prevented deadly anesthetic gas explosions by reducing static electricity sparks.54,55,56,57
Hospital layouts influenced patient outcomes by directly influencing nursing and medical care efficiency. Even Nightingale and her followers advised that the number of patients one head nurse could oversee determined the size limit of a pavilion ward.16,58 By the early 20th century, studies measured nursing efficiency using the pedometer. To reduce distances traveled by caregivers in the course of their duties, designers experimented with ward layouts that had standard rooms for patients with shorter and fewer corridors, more centralized nurse stations, improved supervision (via use of glass), and more numerous utility cabinets.9,59,60,61,62,63
Personnel and material shortages during the Second World War prompted hospital practitioners to study efficiencies in all corners of the hospital.64 This focus was evident not only in numerous studies of designs that improved specific services or functions, but also in extensively researched, standardized model plans (called “type” plans) published by the US Public Health Service as a resource to help hospital administrators maximize personnel efficiency, minimize materials used, and improve patient outcomes.65 Postwar hospital efficiency studies incorporated new methods and new concerns, including task-level time and motion studies for doctors, nurses, and staff.66,67,68 The Greater Baltimore Medical Center’s horizontal layout (built at a time when hospital designs were trending vertically) was determined by “operations research” that studied hospital traffic patterns and developed a layout that would make for the most efficient pattern.69 During the 1950s and 1960s, designers regularly based experimental ward unit layouts on evidence gained from construction of full-scale model patient rooms.70,71,72,73,74,75
In operating rooms, standardization of room designs supported standardization of surgical procedures, which reduced infections and minimized the time clinicians needed to spend tending a patient.67,76,77 The ever-changing technologies and procedures of up-to-date surgical practice, however, guaranteed a constant reassessment of both procedures and design features. For example, in the early 1900s, hospitals often included a “recovery” room (often noisy and disruptive) where postoperative patients came out from under anesthesia.78 By the 1930s, recovery rooms were no longer considered best practice, as they required extra handling of the patient.79 In the 1940s, the widely reported improved outcomes for wounded soldiers in military hospital surgical recovery rooms staffed by experienced nurses and stocked with specialized equipment (eg, suction, oxygen) made recovery rooms again essential in postwar surgical suites.78,80 By the 1950s, the success of surgical recovery rooms fueled the spread of intensive care units.
The importance of the effect of patient comfort on outcomes also gained attention in the early 20th century. In 1906, students at Columbia University studied the sources of external noise around a hospital, and their findings became the basis for the creation of hospital quiet zones.81 With the development of color theory, designers decried the negative influence of the ubiquitous all-white hospital surfaces and suggested the beneficial influence of colors.82,83,84 Opportunistic paint manufacturers soon published pamphlets describing which paint colors were best for a room based on exposure (north or south light) and patient ailment.85 By the 1940s, modernist architect Alden B. Dow incorporated a color scheme designed to provide a positive, more cheerful, patient experience in Midland Hospital in Michigan. Each room provided a therapeutic view of natural surroundings and incorporated its own unique color balance to promote a positive response, with softer, more restful, colors for design elements (eg, dark green floors, light green walls, blue ceilings, and pink woodwork) in patient rooms and more brilliant, stimulating colors for design elements (eg, orange-red floors, white walls, and green ceilings) in public spaces.86,87 Postoccupancy qualitative surveys quoted patients as commenting that “It’s a beautiful place to be sick in, if you have to be sick.”88 Similar attention to the positive effects of art and music on patient outcomes brought all sorts of new entertainments and distractions to the mid-century patient’s bedside.89,90,91
By the 1960s, new strategies of gathering data on patient experiences fueled the new field of architectural psychology and many resultant design refinements.92 In Topeka, Kansas, a new environmental research building even offered a complete spatial laboratory for studying architectural variables and their effects on patients.93
The above examples show that evidence has provided a basis for hospital design for decades. One additional example will show how deep that history might go within each example.
Early 20th-century obstetric unit designs included sterile formula rooms (which were designed at the level of aseptic detail of the surgical suite) and centralized nurseries, which could hold dozens of infants and which typically required gowning and masking for access (see Figure 5).94,95 This layout was intended to reduce infections, but it also reduced infant-parent interactions.
Figure 5. US Public Health Service Type Plan of Central Nursery Layouta
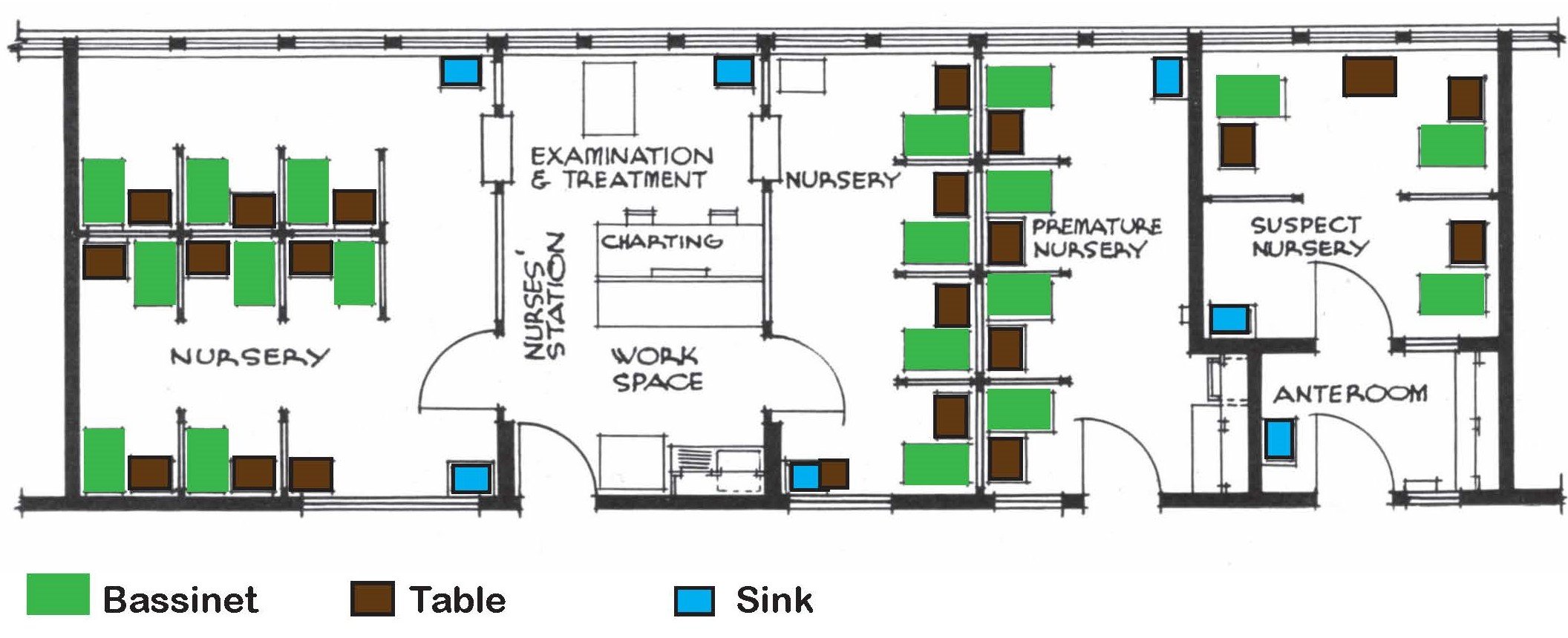
Plan reproduced from Dunham et al,94 with graphic indications of bassinets, sinks, and tables added by author.
a For hospital expecting 700 live births per year.
In the early 1940s, the Cornelian Center of Detroit—citing literature that showed behavioral problems could stem from infancy—redesigned its childbirth suites to house the infant in the same room with the mother and reported increased bonding between parents and infant, encouragement of breastfeeding over formula feeding, reduced crying, and reduced nursing load.96 To gather more data, the George Washington University Hospital included several different nursery and maternity room designs in a new maternity facility in 1945 (see Figure 6). Postoccupancy analyses summarized the benefits of each layout but led to the general conclusion that smaller nurseries in greater proximity to the mother reduced infection, increased mother-baby interaction, and encouraged breastfeeding over formula feeding.97
Figure 6. Rooming-in Layouts

Graphic by author, based on Mongomery TL, Keast M.98
By 1948, the Grace-New Haven Community Hospital in Connecticut reported numerous positive outcomes (happier mothers, healthier babies, more efficient nursing, and—though inconclusive because of the small sample size—possibly fewer infections) associated with its experimental rooming-in unit (see Figure 6).99 Over the next few years, rooming-in suites appeared in hospitals across the country, each reporting positive outcomes. 98,100,101,102,103,104,105
Modern EBD is understood as an active and intentional research process involving the gathering, analysis, and publication of data on which to base design decisions.1 In each of the historical examples presented above, the designers followed that process. If there is a clear difference between EBD then and now it is in the greater present emphasis on the methodological and analytical framework of the research.
If hospital designers have been basing designs on evidence for decades, architects more generally only began to express awareness of how little they knew about the effects of their designs on the occupants in the 1950s.92,106,107,108,109,110 Conscious attempts to incorporate research as a basis for design gained traction in professional architectural circles beginning in the 1960s. 111,112,113,114,115 Since then, evidence-based architectural research has grown ever more sophisticated, more detailed, more rigorous, and more central to the profession. Situated in this larger context, Ulrich’s 1984 publication and the development of EBD becomes part of a much larger, much longer transformation of design. The examples given in this article suggest the extent of the history that is still waiting to be told.
About EBD. Center for Health Design. Accessed December 30, 2023. https://www.healthdesign.org/certification-outreach/edac/about-ebd
Levin D. Evidence-based design origins. Healthcare Design Mag. May 20, 2014. Accessed May 30, 2024. https://healthcaredesignmagazine.com/trends/architecture/evidence-based-design-origins/?hilite=evidence-based+design+origins
Mitchell E. Hospitals and evidence-based design part 2: the revolutionary 100 years. EOSCU blog. March 25, 2022. Accessed May 30, 2024. https://blog.eoscu.com/blog/hospitals-and-evidence-based-design-part-2-the-revolutionary-100-years
Tenon J. Memoirs on Paris Hospitals. Science History Publications; 1997.
Howard J. An Account of the Principal Lazarettos in Europe; With Various Papers Relative to the Plague: Together With Further Observations on Some Foreign Prisons and Hospital; and Additional Remarks on the Present State of Those in Great Britain and Ireland. 2nd ed. J Johnson, C Dilly, & T Cadell; 1791.
Tilton J. Economical Observations on Military Hospitals: And the Prevention and Cure of Diseases Incident to an Army: In Three Parts: Addressed I to Ministers of State and Legislatures, II to Commanding Officers, III to the Medical Staff. J Wilson; 1813.
Kisacky JS. Rise of the Modern Hospital: An Architectural History of Health and Healing, 1870-1940. University of Pittsburgh Press; 2017.
Bruegmann R. Architecture of the Hospital, 1770-1870: Design and Technology. Dissertation. University of Pennsylvania; 1976.
Kisacky J. Breathing room: calculating an architecture of air. In: Gerbino A, ed. Geometrical Objects: Architecture and the Mathematical Sciences 1400-1800. Springer; 2014:247-280.
Sylvester C. The Philosophy of Domestic Economy: As Exemplified in the Mode of Warming, Ventilating, Washing, Drying and Cooking, Contributing to the Comfort of Domestic Life. Barnett; 1819.
Some Account of the Medical School in Boston, and of the Massachusetts General Hospital. Phelps & Farnham; 1824.
Watson J. Thermal Ventilation, and Other Sanitary Improvements, Applicable to Public Buildings, and Recently Adopted at the New York Hospital: A Discourse, Delivered at the Hospital, February 8th, 1851. Wm W Rose; 1851.
Nightingale F. Notes on Hospitals. 3rd ed. Longman, Green, Longman, Roberts, & Green; 1863.
Thompson JD, Goldin G. The Hospital: A Social and Architectural History. Yale University Press; 1975.
Taylor JRB. The Architect and the Pavilion Hospital: Dialogue and Design Creativity in England 1850-1914. Leicester University Press; 1997.
New York Hospital Building Committee. Report of the Building Committee: Together With an Address Delivered on the Occasion of the Inauguration of the New Building, on the 16th March, 1877. LW Lawrence; 1877.
Billings JS. Johns Hopkins Hospital: Reports and Papers Relating to Construction and Organization. No. 5, on Heating and Ventilation. Wm K Boyle & Son; 1878.
Billings JS. Description of the Johns Hopkins Hospital. Isaac Friedenwald; 1890.
A Laboratory Technist. Infections caused by “slips” in operating room technic. Mod Hosp. 1915;5(6):411-413.
Smith S. Principles of Hospital Construction. Trustees of the Roosevelt Hospital; 1865.
Pfeiffer C. A report upon “sanitary relations to health principles of architecture.” Public Health Pap Rep. 1873;1:147-156.
Adams A. Medicine by Design: The Architect and the Modern Hospital, 1893-1943. University of Minnesota Press; 2008.
Finest hospital in the world. New York Times. December 1, 1912. Accessed May 30, 2024. https://www.nytimes.com/1912/12/01/archives/finest-hospital-in-the-world-in-cincinnati-elaborate-plant-on-the.html
Hospital’s strong ally—an open air roof ward, experiment at the Presbyterian Institution a success. New York Times. December 9, 1906. Accessed May 30, 2024. https://www.nytimes.com/1906/12/09/archives/hospitals-strong-ally-an-open-air-roof-ward-experiment-at-the.html
Pneumonia being conquered in the open air, instead of hot rooms and equal temperature, the hospital roof and the winter’s blast are utilized with success in the treatment of this scourge. New York Times. January 26, 1908. Accessed May 30, 2024. https://www.nytimes.com/1908/01/26/archives/pneumonia-bieng-conquered-in-the-open-air-instead-of-hot-rooms.html
Short CA. The Recovery of Natural Environments in Architecture: Air, Comfort and Climate. Taylor & Francis; 2017.
Galton SD. Healthy Hospitals. Observations on Some Points Connected With Hospital Construction. Clarendon Press; 1893.
Operations research helped shape this hospital design. Mod Hosp. 1966;107(5):122-125.
Pflueger MT; Skidmore Owings & Merrill Associated Architects. Structural details of model room, Mount Zion Hospital, San Francisco. Mod Hosp. 1948;71(3):62-63.
Se D, Holzinger KJ Jr, Bachmeyer AC; Erhart Eichenbaum & Rauch Architects. 600-bed general hospital in Arkansas changes the health map. Archit Forum. 1950;93(1):90-95.
Gorschalki R, Bird T. Two-bed unit simplifies operation. Mod Hosp. 1950;75(5):81.
Doane JC. Is standardization of surgical technique possible? Mod Hosp. 1931;36(1):81-84.
Markus FE. Time and motion studies in the operating suite. Mod Hosp. 1952;78(6):80-81.
Hannaford HE. Planning the general hospital. Archit Forum. 1932;57(5):319-398.
Wawro NW. The recovery room has much to recommend it. Mod Hosp. 1949;73(5):64.
Rice MIL. Law aids the hospitals. New York Times. December 6, 1907. Accessed May 30, 2024. https://www.nytimes.com/1907/12/06/archives/law-aids-the-hospitals-its-hand-stretched-out-to-make-quiet-around.html
Midland Hospital by Alden B. Dow. Alden B. Dow Home & Studio. November 11, 2022. Accessed 13 July 2024, 2024. https://www.abdow.org/midland-michigan-hospital-alden-dow/
Action by the auxiliary makes children’s ward a fairyland. Mod Hosp. 1949;72(3):92-94.
Knoblauch J. Architecture of Good Behavior: Psychology and Modern Institutional Design in Postwar America. University of Pittsburgh Press; 2020.
US Public Health Service Hospitals Facilities Section. Notes on hospital planning. Archit Rec. 1946;100(2):101-116.
Garfield SR. Permanente has the answer to living-in problems. Mod Hosp. 1951;77(1):61.
What should be the logic of the way we plan our hospitals for the people? A modern hospital round table. Mod Hosp. 1966;106(3):114-122, 164-170.
Stainbrook E. Architects not only design hospitals: they also design patient behavior. Mod Hosp. 1966;106(3):100.
Evans BH. What is research for architecture? AIA J. 1964;41(5):87-89.



