Art of Medicine
Jul 2022
Peer-Reviewed
In arts-based-research, knowledge and meaning emerge from people’s experiences of being in dynamic, ambiguous, intentional, and ethical relationships with each other and the arts. This case study draws on Launer’s “7 C’s” (context, conversations, curiosity, complexity, challenge, caution, and care) to understand the aesthetics (shape and form) and ethics of relationships between an artist-researcher and patient-sitter in portraiture-based medical research. This case supports the 7 C’s being embodied in the art-making process, as the approach can usefully frame ethical challenges and rewards of portraiture-based health research for artist-researcher and patient-participant.
Ethics of care (EoC) is a normative ethical framework that views moral action in terms of interpersonal relationships, with care and benevolence as core virtues. Because this ethical framework reflects the relationship between carers and patients, we decided to explore its usefulness for artist-sitter and researcher-participant relationships in a portraiture-based medical research (PBMR) study.1
Launer has proposed that context, conversations, curiosity, complexity, challenge, caution, and care (the “7 C’s”) can help scholars understand the relationships between doctors and patients.2,3 Since many of these themes overlap with EoC, we decided to use Launer’s 7 C’s to explore the EoC in the interactions and relationships between the first author—Scottish artist-researcher, Mark Gilbert (M.G.)—and sitter-participant, Lawrence. This case report was drawn from the Giving, Receiving, Observing and Witnessing Care (GROWing Care) Study, which investigated the experience of older adults and their partners in care.4 We examined artworks, transcripts from conversations, and semi-structured interviews between artist-researcher and sitter-participant, as well as artist journal reflections.
M.G. met Lawrence, then 91 years old, after Lawrence’s appointment at a memory clinic for subjective memory complaints. Although Lawrence’s test results showed no sign of dementia, his geriatrician asked him to consider participating in the GROWing Care Study.4 Lawrence had painted with watercolors, was curious about the study, and consented. From 2018 to 2020, M.G. and Lawrence worked on a series of portraits recording Lawrence’s life journey—from his leaving England (see Figure 1), to his immigration to Canada, through the emotional journey of grieving the unexpected deaths of his wife, Dorothy, and oldest daughter, Penny.
Figure 1. Lawrence in his 20s, as a Competitive Road Cyclist in England

Photographer unknown; courtesy of Lawrence.
Photograph.
Lawrence shared stories about his past, future, health, illnesses, loves, and losses. For example, M.G. learned that, following the deaths of Dorothy and Penny, Lawrence stayed with his younger daughter, Patricia, and her family. Patricia, as Lawrence’s primary caregiver, also consented to participate in this study and sat for M.G. for her own portraits (see Figure 2).
Figure 2. Patricia, Lawrence’s Younger Daughter, 2018

Courtesy of Mark Gilbert.
Pastel on paper, 35" x 37".
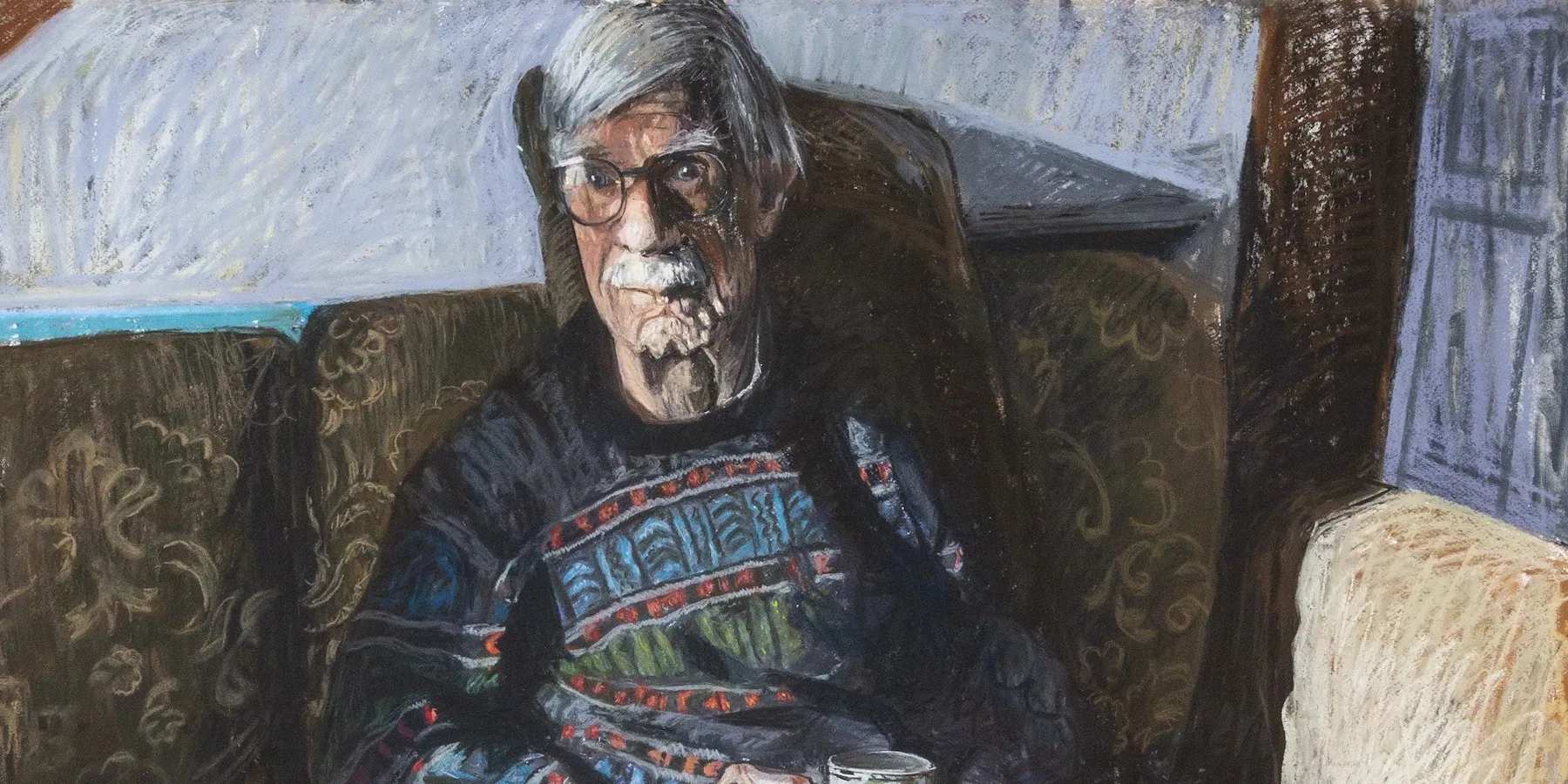
As Lawrence sat, his big hands nervously fiddled with his shirtsleeves (see Figure 3). The rapid intimacy engendered during the initial sitting might have felt somewhat awkward, but it facilitated a more trusting relationship between artist and sitter, both of whom expressed themselves freely. Lawrence shared that Dorothy and Penny had each died of cancer within a few months of each other. Penny, Lawrence explained, following a difficult birth in England, was left with a severe cerebral palsy that prevented her from walking, despite her above-average intelligence. When Dorothy became a powerful campaigner for disability rights in the Canadian Maritimes, Lawrence maintained his primary role as caregiver to Penny.
Figure 3. Portrait of Lawrence at Home, 2018
Courtesy of Mark Gilbert.
Pastel on paper, 63" x 53".
Lawrence often brought the conversation back to Penny. At times, M.G. observed him becoming quite emotional and visibly upset when talking about her. Lawrence’s sorrow and grief seemed to be assuaged by a palpable pride in all that Penny had achieved. Penny lived life to the full, earning a university degree in commerce, getting married, and winning prizes for sports. Lawrence stated, Penny “could do anything … she wanted to do.”
M.G. shared with Lawrence his own story of growing up in Scotland. During the study, M.G.’s father, Norman Gilbert, who was also an artist,5 died, and M.G. often reflected on this loss with Lawrence. Lawrence was the same age as M.G.’s father. Despite the many years difference between Lawrence and M.G., they recognized their shared artistic and UK heritage and their recent bereavements. These conversations illuminated their shared interests and generated greater mutuality as they worked together to make portraits.
Launer described curiosity as “emotional engagement” in “a focused and committed interest in where the story might go.”2 Curiosity was critical to building the relationship between M.G. and Lawrence and to creating the portraits. M.G. noted in his journal: “I continue to measure, and try to maintain a ‘searching’ element to the marks I make, jettisoning all preconceptions ... trying to just respond to Lawrence and the pose.”
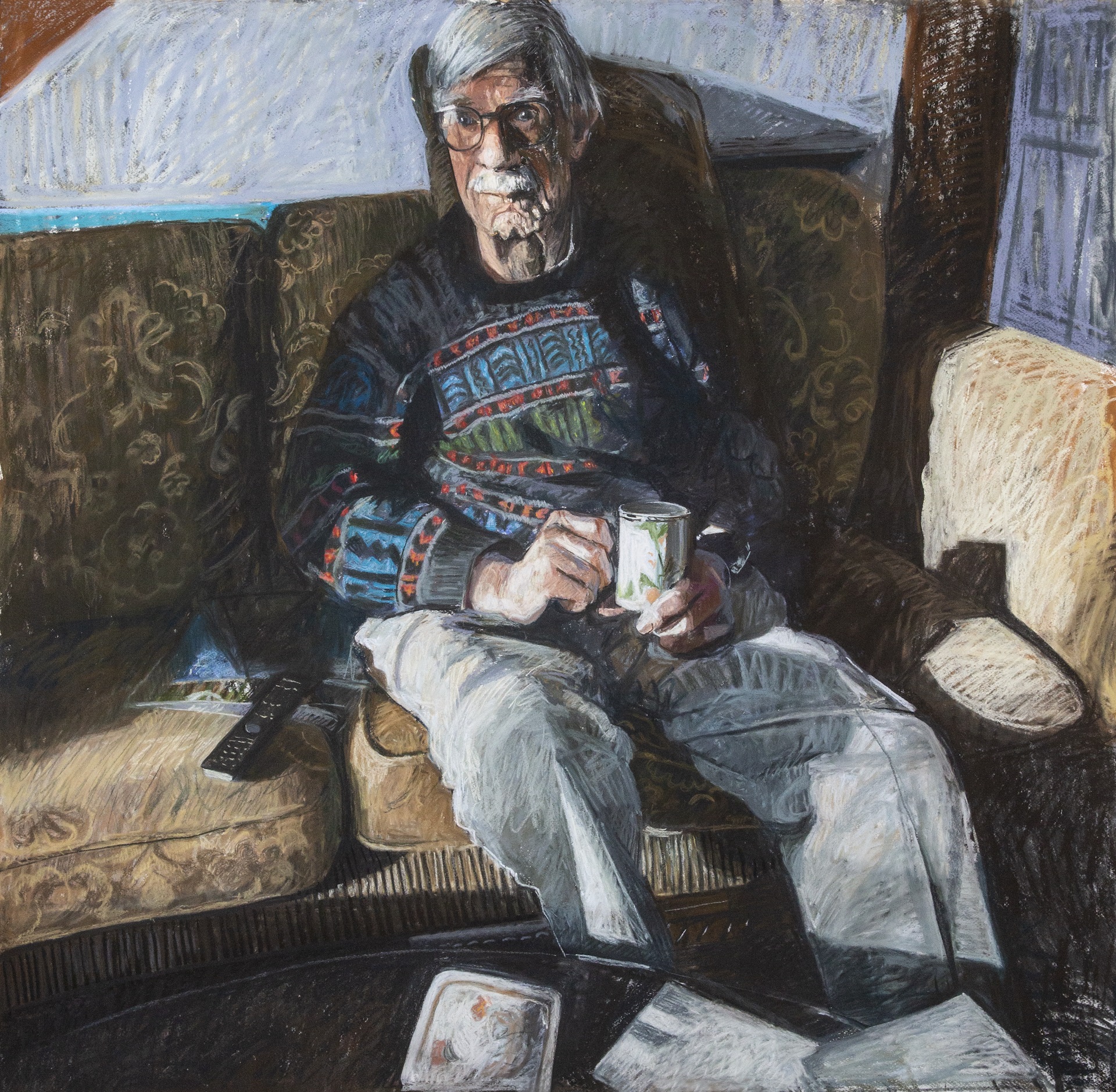
Being positioned in the artistic research process invited Lawrence and M.G. to think about the portraits from different viewpoints. Lawrence noted: “My energy has got your portrait onto the paper ... it guides your hand” (see Figure 4). M.G. journaled: “I tell him [Lawrence] during the next break that I am having problems with the composition and proportions of his portrait. Lawrence seems to relate to my problem, and comes over to look at the drawing and offers me advice ... he suggests that the head is too big for the shoulders, and he feels ‘it is a shame to change the head, because it is good.’” Inquisitively, he went on to say, “sometimes you have to make it wrong so that it looks right.” Their mutual curiosity and openness facilitated co-creation of the portrait.
Figure 4. Lawrence II, 2019

Courtesy of Mark Gilbert.
Pastel on paper, 53" x 51".
Complexity engenders a “an infinite and unpredictable dance of interactions.”2 Both artist and sitter engaged in the process, not knowing the end at the beginning. M.G.’s choice to work in pastel allowed for experimentation and improvisation of a drawing with the color and richness of a painting. M.G. strived for every mark to be an authentic response to Lawrence. Lawrence remarked: “As an artist, I can leave out things that I don’t like, and change things.” However, he recognized that “if you’re trying to do the portrait of my life then there’s something missing.” When M.G. nervously showed the drawings to Lawrence, he responded, “I look sick.” However, M.G. was reassured when, at a later session, Lawrence viewed these portraits again and said, “the whole point … is to be as honest as possible.” Their honesty supported their relationship in co-creating portraits by establishing trust and acknowledging challenges.
Lawrence and M.G. had been working with each other for 9 months when M.G. received a call from Patricia, who said that Lawrence had fallen at home and broken his hip. Initially, Lawrence struggled physically to recover from hip surgery. As is not rare at his age, despite being in reasonably good health, Lawrence experienced early postoperative delirium. Lawrence described how frightening were the hallucinations he experienced and his frustration that nobody took him seriously when he tried to talk about them.
Lawrence felt “despondent” during the early days after the surgery. At times, although he grew tired of talking, he was still happy to be drawn (see Figure 5). As he lay in bed, looking frail and suffering from the effects of his medication, he communicated doubts: “Why do we go through all this…. What’s the point? Is it going to do any good?... Maybe it’s better to ignore it and just keep going. You keep going and then you’re not there, and then everything is just back to normal.” Nevertheless, Lawrence recognized the ever-evolving nature of his story, stating: “Tomorrow I’ll probably change and move on from this despondency.”
Figure 5. Portrait of Lawrence in Hospital Following His Fall, Recovering From His Surgery, 2019

Courtesy of Mark Gilbert.
Pastel on paper, 63" x 53".
In his journal, M.G. wrote: “even the challenges and discomfort I feel while making the drawing, are instilled with fears that I am able to share and overcome with Lawrence.” Practicing caution, M.G. monitored his own and Lawrence’s emotional responses and recognized when to stop questioning, stop probing, and stop analyzing.1 Working in a clinical context required M.G. to practice reflexivity, sensitively reflecting on his role in his interactions with Lawrence, while maintaining a mindful awareness of Lawrence’s needs and willingness to continue to engage. M.G.’s fears as he started each portrait were tempered by the presence of Lawrence. Together, the two negotiated the boundaries of the research and the art.
Launer wrote: “None of the ‘C’s’ will work in the way intended unless the person applying them is careful, attentive and kind.”1 Care is at the heart of the practice of medicine and, in our opinion, was central to the interactions in this PBMR project. In his journal M.G. wrote: “I am sure that the sharing and collaboration in the [portrait] process is full of compassion.” For both artist and sitter, the portraiture process created a relationship in which care for one another and for the images themselves was foundational to their partnership. We subscribe to Lawrence-Lightfoot and Davis’ statement that “it is in the building of relationships that the portraitist experiences most pointedly the complex fusion of conceptual, methodological, emotional and ethical challenges.”6
Attending carefully to relationships is foundational to EoC or any work of co-creation. EoC centers on clinical interactions, which can engender co-creation of knowledge, to improve outcomes and satisfaction with care.7 Recognizing the 7 C’s not only in doctor-patient relationships in health care, but also in artist-sitter or researcher-participant relationships—particularly in portraiture-based medical research—can help those involved in the interactions to develop relationships that support a more ethical creative process and can lead to mutual understanding, richer findings, and more valuable outcomes.7,8,9
Launer J. Narrative-Based Practice in Health and Social Care: Conversations Inviting Change. 2nd ed. Radcliffe Medical Press; 2018.
Gilbert N. Norman Gilbert. Accessed October 6, 2020. https://www.normangilbert.com/
Lawrence-Lightfoot S, Davis JH. The Art and Science of Portraiture. Jossey-Boss; 1997.
Kuipers SJ, Cramm JM, Nieboer AP. The importance of patient-centered care and co-creation of care for satisfaction with care and physical and social well-being of patients with multi-morbidity in the primary care setting. BMC Health Serv Res. 2019;19:13.
Jull J, Giles A, Graham ID. Community-based participatory research and integrated knowledge translation: advancing the co-creation of knowledge. Implement Sci. 2017;12:150.