History of Medicine
Dec 2024
The establishment of the American Medical Association in 1847 launched medical practice standardization in the United States. Consensus on standards was hard won, however, and implementation was not immediate. Hospital design standards, specifically, were debated for decades and were ultimately ceded to nurses and architects. This article describes key moments along that trajectory.
In the 1800s, hospitals’ designs were more products of trial and error than evidence based. Physicians then were the most frequent occupiers of hospitals, so they were well placed to share their insights about design features. The American Medical Association (AMA) and other physicians’ groups got to work on establishing medical standards and guidelines but didn’t directly engage in designing hospital structures and spaces. Decades after the founding of the AMA in 1847, AMA members and health care organizations continued to ask key questions about hospital design: How many stories should a hospital be?1 What is the best method of ventilation?2 Is a handwashing station really necessary?3
The beginnings of the first public hospital in the United States dates back to the 1600s.4 Early hospitals had a very poor reputation, and any patients who could afford it were treated at home.5 The first hospitals in the United States mainly served the military and the indigent (public hospitals grew out of almshouses4)—in other words, people without a choice. Generally, hospitals were viewed as dangerous bastions of infection and disease.5 Diseases like puerperal fever spread like wildfire through lying-in hospitals, as surgeons would perform autopsies in the morning and deliver babies in the afternoon without washing their hands.6 Even into the mid-19th century, hospital buildings were poorly ventilated,7 overcrowded8 and, due to the general lack of hygiene, smelled so terrible that nurses took to wearing perfumed masks.9 Hospitals were built without planning—some had very few windows, no lavatory and bathing facilities (as well as no proper drainage where these did exist), inadequate kitchens, and nowhere for doctors to see patients privately.8
A report presented to the Medical Society of the State of New York in 1863 claimed that though these institutions were created with the best of intentions, they had not only failed to accomplish their goals but in many cases “aggravated the very evils they were designed to remove.”8 Florence Nightingale, a pioneer in hospital sanitation, publicly wondered whether “a succession of temporary sheds” would be safer than the buildings used as hospitals at the time.10 It was largely due to her influence that hospitals began implementing sanitation protocols and evidence-based design in the 1850s.10
In 1854, Nightingale was sent to reform a hospital for injured British soldiers in Crimea where dire conditions caused many unnecessary deaths. Not only did she improve conditions, but she “collected, compiled and communicated statistical data back to Britain to prove the worth of what her team was doing.”11 Her interventions were simple12: avoid overcrowding; provide a clean environment with healthy food, fresh linens and uncontaminated water; use data to make decisions about hospital design13; improve air circulation14; and practice good waste management.
Once Nightingale returned to England, she set about solving some of the major issues facing medical professionals of the day. She recommended the complete redesign of entire hospital floors, providing “detailed notes on how to determine the correct amount of space surrounding each bed, accounting for ventilation, administration and clinical instruction.”14 She advocated for pavilion style hospitals, which predominated during the latter half of the 19th century, to reduce the spread of infection and provide better ventilation.14 This style of hospital architecture featured elongated, narrow sections with multiple windows located in opposing pairs for cross-ventilation, promoting enhanced airflow and increased efficiency in treating patients with similar injuries or illnesses. While most hospitals were designed like hotels, the pavilion style was more like a tent, its structure offering sufficient ventilation while safeguarding against harsh weather conditions. Frequently interconnected by a shared passageway, this layout also had the benefit of facilitating hospital staff’s swift access to any pavilion ward.14
One of the innovations included in this plan was to have a “clean area” at one end of the hospital wing and a “dirty area” at the other end. As Campbell explains, “The clean end would contain the entrance(s), nurse’s dayroom, scullery, storeroom, linen closet, coat closet, private watercloset, and staircase, if any. The dirty end would include the patients’ watercloset, lavatories, sinks, and a separate ante-room located prior to the former spaces.”15 Nightingale’s recommendations were exceptionally detailed, specifying which materials should be used for furniture and flooring, which direction pavilions should face for optimal natural light, and which heat sources should be used.16
Nightingale was not the only one in the medical field to make these discoveries in the mid-19th century. AMA members were similarly discovering the importance of proper ventilation in hospital design at around the same time. As early as 1848, AMA members provided testimony proving that “two of the most alarming and fatal scourges of humanity, typhus and puerperal fevers, are intimately connected with, and in a great degree dependent upon, accumulations of filth, and impure atmosphere, and that their ravages are immediately under the control of sanitary measures, and may be checked by a faithful compliance with proper legislative enactments.”16 In 1851, AMA members discussed the importance of thermal ventilation in patient care.2 An 1864 report in the Transactions of the American Medical Association notes that, for wounded soldiers, fresh air and distance from “suppurating wounds” were found to be perhaps the most effective methods of recovery.17 The next year, the Committee on Military Hygiene issued a report on faulty construction and selection of hospital buildings, which included ventilation plans (see Figure 1).1 When hospitals were thought to be well constructed, members of the AMA were invited to tour their facilities,18 presumably so the hospital administrators could share their methods with a wide audience capable of advocating for them. Later, when the Journal of the American Medical Association was created in 1883, articles on new hospital designs and descriptions of existing hospitals popped up from time to time, but by this time the field of hospital design had been outsourced to architects and administrators.
Figure 1. Illustrations of the Effects of Hospital Ventilation Plans
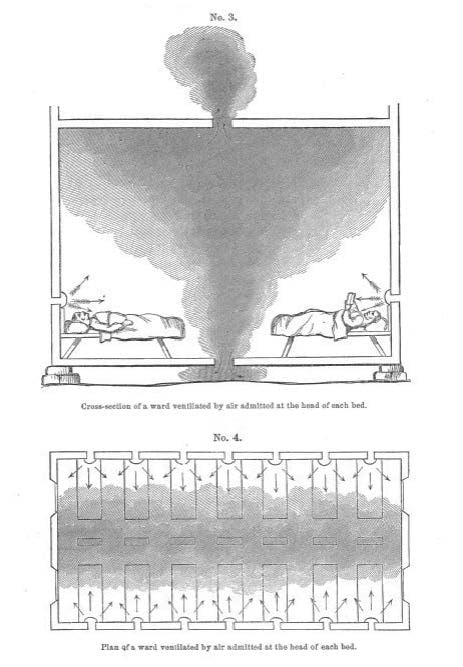
Reproduced from American Medical Association.1
This diagram was presented at the AMA’s Annual Meeting in 1865. It shows how different methods of ventilation moved “foul air” around the hospital ward.
The AMA’s position on its role in hospital design is best summed up in an 1859 address to the House of Delegates. Dr Harvey Lindsly stated:
The importance of ventilation to comfort, health, and life, can hardly be overrated, and to medical science is almost exclusively due whatever improvement has been made in this respect in our public and private edifices. A vast deal, to be sure, yet remains to be done, but this must rest with architects, builders, and the people themselves, after the evils of breathing impure air have been so often and so thoroughly exposed by the profession.19
The AMA also believed that hospital sanitation was best dealt with by nurses rather than physicians. In an 1869 report on the training of nurses, it is said that a nurse’s education must consist of the “principles of hygiene”; “methods of preparing food and drink”; “administration of” medicines; “application of leeches, blisters, bandages and other dressings”; and “making up beds, changing sheets, and handling patients exhausted by disease and injury.”20 Despite the overlap between many AMA opinions and Nightingale’s, she is not mentioned in the AMA’s official transactions until 1869, and her specific recommendations are never discussed at all, although the pavilion style hospitals she advocated for were eventually favored by the AMA as well.21 As Figure 2 illustrates, new hospital buildings did not necessarily adhere strictly to Nightingale’s recommendations but incorporated the principles of design she advocated for, including long corridors with distinct wards.
Figure 2. Plan of the Second Floor of the Peterson Hospital in New York
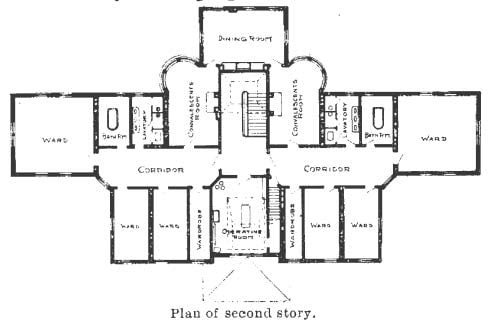
Reproduced from Spratling.22
This floor plan, which appeared in an 1898 article in the Journal of the American Medical Association, shows the second floor of the Peterson Hospital at the Craig Colony for Epileptics. The hospital was designed for the care and treatment of acute medical and surgical cases only, and its capacity was from 20 to 24 beds. The floor plan was submitted to the journal, along with its specifications, by the medical superintendent of the colony.
As medical technology advanced, it became apparent that hospitals—in addition to providing a sterile, comfortable environment—must also be bastions of efficiency, with plenty of room for all the new equipment that was being invented. These demands meant that the pavilion plan was no longer practical. To ensure a window in each room, the buildings couldn’t exceed a width of 2 rooms, leading to the necessity of constructing multiple lengthy and narrow wings. The resulting sprawling structures incurred high construction costs; were excessively expensive to heat, light, and provide water for; and proved inefficient and labor intensive to manage. Time and motion studies were used to determine layouts and locations of different departments, and diagnostic and treatment spaces were redesigned to create more efficient pathways for the movement of supplies, patients, nurses, technicians, and physicians.23
As hospital design became more complicated, physicians and nurses alike played a smaller role in discussions of issues like ventilation and sun exposure, although they often served as consultants to business committees and architects.23 But the AMA’s influence on medical standards continued to contribute to the broader context in which health care professionals and architects collaborated to enhance hospital design and infrastructure.
Andrews E. Report of the Committee on Military Hygiene. Trans Am Med Assoc. 1865;15:167-181. Accessed January 17, 2024. http://ama.nmtvault.com/jsp/PsImageViewer.jsp?doc_id=6863b9b4-a8b5-4ea0-9e63-ca2ed554e876%2Fama_arch%2FAD200001%2F00000015&pg_seq=207
Gaillard PC, Drake D, Emerson G, Desaussure HW. Report of the Committee on Hygiene. Trans Am Med Assoc. 1851;4:517-544. Accessed January 17, 2024. http://ama.nmtvault.com/jsp/PsImageViewer.jsp?doc_id=6863b9b4-a8b5-4ea0-9e63-ca2ed554e876%2Fama_arch%2FAD200001%2F00000004&pg_seq=523
B AR. Letter from Vienna. J Am Med Assoc. 1886;6(12):333-334.
Fiani B, Covarrubias C, Jarrah R, Kondilis A, Doan TM. Bellevue Hospital, the oldest public health center in the United States of America. World Neurosurg. 2022;167:57-61.
Starr P. The Social Transformation of American Medicine: The Rise of a Sovereign Profession and the Making of a Vast Industry. Basic Books; 1982.
Shaikh S. “The Contagiousness of Puerperal Fever” (1843), by Oliver Wendell Holmes. Embryo Project Encyclopedia. July 26, 2017. Updated September 11, 2023. Accessed January 12, 2024. https://embryo.asu.edu/pages/contagiousness-puerperal-fever-1843-oliver-wendell-holmes
Munson A, Wetmore EA, Benedict ND. Eleventh annual report of the managers of the state lunatic asylum: made to the legislature February 8, 1854. Curtiss & White; 1863. Accessed January 12, 2024. https://archive.org/details/b30304714/mode/2up
Lee CA. Remarks on hospital construction, with notices of foreign military hospitals. Trans Med Soc State New York. 1863;225:37-66. Accessed January 20, 2024. https://books.google.com/books?id=dAegAAAAMAAJ&pg=PA37&lpg=PA37&dq=charles+a+lee+%22remarks+on+hospital+construction%22+1863&source=bl&ots=XF7ydNo__z&sig=ACfU3U2KdyeDr2eTgaOqoautmu4KmUdpVg&hl=en&sa=X&ved=2ahUKEwiV1v-s2eeDAxUjHjQIHXbyApEQ6AF6BAgOEAM#v=onepage&q=charles%20a%20lee%20%22remarks%20on%20hospital%20construction%22%201863&f=false
McConnell CR. Hospitals and Health Systems. Jones & Bartlett Learning; 2020.
Bynum WF. Science and the Practice of Medicine in the Nineteenth Century. Cambridge University Press; 1994.
Hollingham R. The pioneering surgeons who cleaned up filthy hospitals. BBC. August 19, 2020. Accessed January 25, 2024. https://www.bbc.com/future/article/20200812-the-pioneering-surgeons-who-cleaned-up-filthy-hospitals
Karimi H, Masoudi Alavi N. Florence Nightingale: the mother of nursing. Nurs Midwifery Stud. 2015;4(2):e29475.
Campbell WT. Pavilion-style hospitals of the American Civil War and Florence Nightingale. National Museum of Civil War Medicine. July 8, 2019. Accessed January 15, 2024. https://www.civilwarmed.org/surgeons-call/pavilionhospitals/
Wynne J, Thomas JM. Communication on hygiene, from the Medical Department of the National Institute. Trans Am Med Assoc. 1848;1:305-310. Accessed January 17, 2024. http://ama.nmtvault.com/jsp/PsImageViewer.jsp?doc_id=6863b9b4-a8b5-4ea0-9e63-ca2ed554e876%2Fama_arch%2FAD200001%2F00000001&pg_seq=315
Andrews E. Diatheses: their surgical relations and effects. Trans Am Med Assoc. 1864;14:117-137. Accessed January 17, 2024. http://ama.nmtvault.com/jsp/PsImageViewer.jsp?doc_id=6863b9b4-a8b5-4ea0-9e63-ca2ed554e876%2Fama_arch%2FAD200001%2F00000014&pg_seq=119
Tyler G, Hall JJC, May JF, et al. Minutes of the eleventh annual meeting of the American Medical Association, held in the city of Washington, May 4, 1858. Trans Am Med Assoc. 1858;11:9-28. Accessed January 12, 2024. http://ama.nmtvault.com/jsp/PsImageViewer.jsp?doc_id=6863b9b4-a8b5-4ea0-9e63-ca2ed554e876%2Fama_arch%2FAD200001%2F00000011&pg_seq=28
Address of Harvey Lindsly, president of the Association. Trans Am Med Assoc. 1859;12:51-60. Accessed January 12, 2024. http://ama.nmtvault.com/jsp/PsImageViewer.jsp?doc_id=6863b9b4-a8b5-4ea0-9e63-ca2ed554e876%2Fama_arch%2FAD200001%2F00000012&pg_seq=57
Gross SD. Report of the Committee on the Training of Nurses. Trans Am Med Assoc. 1869;20:161-174. Accessed January 12, 2024. http://ama.nmtvault.com/jsp/PsImageViewer.jsp?doc_id=6863b9b4-a8b5-4ea0-9e63-ca2ed554e876%2Fama_arch%2FAD200001%2F00000020&pg_seq=173
Wright MB. Pigmentation: a rare disease among infants. Trans Am Med Assoc. 1875;26:195-217. Accessed January 12, 2024. http://ama.nmtvault.com/jsp/PsImageViewer.jsp?doc_id=6863b9b4-a8b5-4ea0-9e63-ca2ed554e876%2Fama_arch%2FAD200001%2F00000026&pg_seq=219
Kisacky J. When fresh air went out of fashion at hospitals: how the hospital went from luxury resort to windowless box. Smithsonian Mag. June 14, 2017. Accessed January 25, 2024. https://www.smithsonianmag.com/history/when-fresh-air-went-out-fashion-hospitals-180963710/



